ASA warns against multiple patients per ventilator
Sharing mechanical ventilators should not be attempted during the coronavirus disease 2019 (COVID-19) pandemic, according to a joint statement published March 26 by the American Society of Anesthesiologists, Society of Critical Care Medicine, American Association for Respiratory Care, Anesthesia Patient Safety Foundation, American Association of Critical‐Care Nurses, and American College of Chest Physicians.
31 mar 2020--The organizations noted that interest in ventilating multiple patients on one ventilator has been raised by those who would like to expand access to mechanical ventilators during the COVID-19 pandemic. Therefore, the organizations advise clinicians that sharing mechanical ventilators should not be attempted while any clinically proven, safe, and reliable therapy remains available.
The reasons for avoiding ventilating multiple patients with a single ventilator include volumes going to the most compliant lung segments; managing positive end-expiratory pressure would be impossible; monitoring patients and measuring pulmonary mechanics would be challenging or impossible; monitoring and management of alarms would not be feasible; there would be no possibility of individualized management for clinical improvement or deterioration; and in the case of cardiac arrest, ventilation would need to be stopped to all patients to allow the change to bag ventilation without aerosolizing the virus, thereby altering breath delivery dynamics to other patients. In addition, patients may deteriorate and recover at different rates and distribution of gas would be unequal and unmonitored to each patient. The greatest risks occur with sudden deterioration of a single patient, resulting in the balance of ventilation being distributed to the other patients.
Finally, ethical issues must be considered. Although a ventilator can be lifesaving for a single patient, it could result in life-threatening treatment failure for all patients if used on multiple patients.
What does supportive care mean for patients with COVID-19?
by From Mayo Clinic News Network
Credit: CC0 Public Domain
Social distancing helps prevent the spread of COVID-19. Most patients who contract the virus will have mild symptoms. Those at greatest risk of developing severe disease include the elderly and people with underlying conditions, such as heart disease, lung disease, and diabetes. Dr. Clayton Cowl, a pulmonologist and Chair of Mayo Clinic's Division of Preventive, Occupational and Aerospace Medicine, says there is no cure or proven treatment for COVID-19, although early clinical studies have shown promise for several medications. The first-line treatment at this time is supportive care, which can help sick patients endure the disease.
What do the terms 'supportive treatment' or 'supportive therapy' mean?
31 mar 2020--"Supportive treatment refers to what we can do to relieve the symptoms of COVID-19," says Dr. Cowl. "By closely monitoring patients, helping them breathe, delivering intravenous fluids, keeping their fever down and treating cough, we can hopefully prevent adverse events, such as chronic shortness of breath, or worse, death in severe cases. But as the number of severe cases increases, we must prepare for delivering supportive care to more people with the illness"
Supportive care to help patients breathe
"Supportive treatment, what's that?" asks Dr. Cowl. "Sometimes we have to provide extra oxygen, supplemental oxygen. Sometimes it involves actually applying something called 'bidirectional positive airway pressure' or even putting someone on a mechanical ventilator temporarily for those who are extremely ill. Most people don't require that level of support."
Why patients may need help breathing
"As with any type of infection, the virus that causes COVID-19 can prompt a large inflammatory response within the lungs themselves," says Dr. Cowl. "This causes you to have difficulty with oxygenation. You may feel as if
you're at the bottom of a pool and can't get to the top fast enough. You feel short of breath because the parenchyma, or the spongy part of the lung, is being affected. You can develop this not only from COVID-19, but any type of viral pneumonia or bacterial pneumonia."
Other types of supportive care:
"It's making sure that you stay adequately hydrated," says Dr. Cowl. "Its making sure your blood pressure doesn't get low because you're getting dehydrated. It's giving medicines to keep your temperature down. Supportive treatment for COVID-19 is similar to treatment for any severe flu symptoms."
Supportive treatment at home
People with mild symptoms of COVID-19 require self-isolation and treatment at home. Dr. Cowl says these supportive treatments may help reduce symptoms.
Resting
Staying hydrated
Monitoring temperature
Consulting health care providers about taking over-the-counter medications
Covering cough and sneezes
Maintaining a distance of at least six feet from other family members
Washing hands regularly
Disinfecting surfaces
Self-isolating from others at home
Avoiding sharing utensils
Considering using paper or disposable products for eating
If your symptoms worsen, consult your health care provider. If emergency symptoms develop, seek emergency medical care.
Emergency symptoms include:
Difficulty breathing
Extremely high temperature, 103 F or above
Chest pain or pressure
Confusion
Severe cough with choking
Blue lips or face
Mayo Foundation for Medical Education and Research
COVID-19 linked to cardiac injury, worse outcomes for patients with heart conditions
COVID-19 can have fatal consequences for people with underlying cardiovascular disease and cause cardiac injury even in patients without underlying heart conditions, according to a review published today in JAMA Cardiology by experts at The University of Texas Health Science Center at Houston (UTHealth).
31 mar 2020--Experts have known that viral illnesses such as COVID-19 can cause respiratory infections that may lead to lung damage and even death in severe cases. Less is known about the effects on the cardiovascular system.
"It is likely that even in the absence of previous heart disease, the heart muscle can be affected by coronavirus disease," said Mohammad Madjid, MD, MS, the study's lead author and an assistant professor of cardiology at McGovern Medical School at UTHealth. "Overall, injury to heart muscle can happen in any patient with or without heart disease, but the risk is higher in those who already have heart disease."
The study authors explained that research from previous coronavirus and influenza epidemics suggest that viral infections can cause acute coronary syndromes, arrhythmias, and the development of, or exacerbation of, heart failure.
In a clinical bulletin issued by the American College of Cardiology, it was revealed that the case fatality rate of COVID-19 for patients with cardiovascular disease was 10.5%. Data also points to a greater likelihood that individuals over the age of 65 with coronary heart disease or hypertension can contract the illness, as well experience more severe symptoms that will require critical care.
According to the study authors, critical cases are those that reported respiratory failure, septic shock, and/or multiple organ dysfunction or failure that resulted in death. "It is reasonable to expect that significant cardiovascular complications linked to COVID-19 will occur in severe symptomatic patients because of the high inflammatory response associated with this illness," said Madjid, who also sees patients at the UT Physicians Multispecialty—Bayshore clinic.
The novel virus that causes COVID-19 was first identified in January 2020. This novel virus originated in Wuhan, China, and by March 11, 2020, the World Health Organization had declared it a global pandemic. The three most common symptoms of COVID-19 include fever, cough, and shortness of breath. Other less common symptoms are muscle pain, sore throat, nasal congestion, and headache. Symptoms can appear as soon as two days after exposure to the virus to up to14 days after. There is a high viral load in both symptomatic and asymptomatic patients, meaning asymptomatic spread between person to person is likely.
Previously identified coronaviruses known to cause severe illness in humans include Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and Middle East Respiratory Syndrome (MERS-CoV). SARS-CoV was first identified in southern China in 2002, and by 2003 it had killed over 8,000 individuals in 29 countries. Data suggests that SARS-CoV may have resulted in cardiovascular complications, such as acute coronary syndrome and myocardial infarction. MERS-CoV was first discovered in 2012 in Saudi Arabia. As of 2019, 2,494 cases have been confirmed along with 858 deaths in 26 countries.
Current COVID-19 treatment options are being researched, and there is a large effort to develop vaccines for prevention and to test antivirals for the treatment of the disease. In the meantime, the study authors encourage all individuals to consult with their health care providers about being vaccinated against influenza and that at-risk patients seek advice on receiving a pneumonia vaccine from their primary care physician. While these vaccines will not provide specific protection against COVID-19, they can help prevent superimposed infections alongside COVID-19.
UC Davis Health has two clinical trials underway for hospitalized patients with severe COVID-19, the disease caused by the novel coronavirus, SARS-CoV-2.
28 mar 2020--The studies are evaluating the safety and effectiveness of two drugs—the investigational antiviral remdesivir, and sarilumab, adrugthat blocks the body's acute inflammatory response.
"We have a critical need to confirm safe and effective treatments for COVID-19," said Allison Brashear, dean of the UC Davis School of Medicine. "Although some patients with severe infection have received remdesivir, we do not have solid data to indicate it can improve clinical outcomes for everyone. The nation's schools of medicine have the expertise and resources to advance knowledge about the infection to help guide the clinical care of patients worldwide."
There are no specific therapeutic agents approved by the Food and Drug Administration (FDA) to treat people with COVID-19. The infection can cause mild to severe respiratory illness. Symptoms can include fever, cough and shortness of breath. Current clinical care of hospitalized patients include supplemental oxygen therapy, antibiotics, influenza antiviral drugs and intensive care as needed.
As of March 26, there were 526,006 confirmed cases of COVID-19 worldwide, including 68,440 in the U.S. and 3,006 in California. There were more than 23,721 deaths, including 994 deaths in the U.S. and 65 in California.
Remdesivir study
UC Davis is one of approximately 75 sites worldwide evaluating the benefits of remdesivir for severe COVID-19 infection. Remdesivir is an investigational broad-spectrum antiviral treatment developed by Gilead Sciences Inc. It was previously tested in humans with Ebola virus disease and has shown promise in animal models for treating Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS), which are caused by other coronaviruses.
UC Davis physicians used remdesivir in February, with emergency approval from the Food and Drug Administration, to treat a critically ill patient who was the first known case of community-acquired infection in the U.S. The patient has since returned home to recover.
The study will enroll up to 440 patients over the next several months, including about 10 or more at UC Davis. Among other criteria, participants must be 18 years of age or older, have a confirmed SARS-CoV-2 test and poor lung function.
The clinical trial is funded by the National Institute of Allergy and Infectious Diseases. It is part of the study recently launched at the University of Nebraska. Stuart Cohen is leading the investigation at UC Davis. He is chief of the Division of Infectious Diseases in the Department of Internal Medicine at UC Davis Health and director of Hospital Epidemiology and Infection Control.
Sarilumab study
UC Davis is one of up to 50 sites in the U.S. assessing sarilumab, a drug jointly developed by Regeneron and Sanofi pharmaceutical companies for the treatment of rheumatoid arthritis. The drug is a human monoclonal antibody that blocks the receptor for interleukin-6 (IL-6), a cytokine that plays an important role in the body's immune response and in generating fever and acute inflammation. The study will evaluate whether the drug can control the progression of the inflammatory response in the lungs of patients with severe COVID-19 infection.
Approximately 400 hospitalized patients age 18 and older with acute COVID-19 infection can be enrolled in the study nationwide. Individuals will be grouped according to the severity of their illness and progression of symptoms, from severe to critical to having multi-system organ failure as well as whether cortisone drugs were used to reduce inflammation. The researchers will be determining whether the health of individuals with high IL-6 levels and severe/critical levels of infection improve with the drug.
The study is sponsored by the U.S. Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response. Timothy Albertson, professor and chair of the Department of Internal Medicine, is leading the study at UC Davis.
Clinical studies essential
Both studies are double-blind, meaning trial investigators and participants will not know who is receiving the treatments. They are designed to identify the early signs of clinical benefit while avoiding the use of ineffective therapies in critically ill patients with COVID-19.
"Conducting well-controlled, randomized clinical trials enable us to confirm the safety and effectiveness of promising drugs to treat emerging infections like COVID-19," Albertson said.
An independent data and safety monitoring board (DSMB) also will closely monitor ongoing results to ensure patient well-being and safety as well as study integrity. The board also will recommend that a study be halted if there is clear and substantial evidence of a treatment difference between drug and placebo.
Provided by UC Davis
What is chloroquine and could it cure the coronavirus?
by Issam Ahmed
Could these pills help solve the coronavirus crisis? Experts are studying Nivaquine (L), which contains chloroquine, and Plaqueril, which contain hydroxychloroquine
Could a pair of decades-old, relatively inexpensive drugs be the solution to the novel coronavirus pandemic?
28 mar 2020--Around the world, countries are expanding access to hydroxychloroquine (HCQ) andchloroquine(CQ), related compounds that are synthetic forms of quinine, which comes from cinchona trees and has been used for centuries to treat malaria.
HQ which is the less toxic of the two, is also used as an anti-inflammatory to treat conditions like rheumatoid arthritis and lupus, purposes it is primarily known for outside the tropics.
The medicines have shown early promise against the COVID-19 illness in early studies in France and China, which led US President Donald Trump this week to call them a "gift from God"—even as experts urge caution until bigger trials validate their effectiveness.
Here is what you need to know.
Why they might work
China used CQ on a trial of 134 patients in February, finding it was effective in reducing the severity of the illness, according to officials.
But these results haven't yet been published. Chinese respiratory expert Zhong Nanshan, who leads a government task force in response to the epidemic, said in a press conference last week that the data would be widely shared soon.
In France, a team led by Didier Raoult of the IHU-Mediterranee Infection, Marseille reported last week they had carried out a study on 36 COVID-19 patients, finding that HCQ drastically reduced the viral load in a group which received the drug.
The effects were especially pronounced when it was used with azithromycin, a common antibiotic used to sweep out secondary bacterial infections.
Medical workers wearing hazmat suits as prevention against the COVID-19 coronavirus at work at the Huanggang Zhongxin Hospital in Huanggang, in China's central Hubei province
What's more, HCQ and CQ drugs have been proven to act against the SARS-CoV-2 virus in lab settings, and a paper published by a Chinese team last week in Cell Discovery offered a potential mode of action.
Karine Le Roch, a professor of cell biology at the University of California, Riverside, explained that both HCQ and CQ are weak bases that elevate the pH of parts of human cells called organelles—which are analogous to organs in animals—and which are normally acidic.
This in turn interferes with the virus' ability to enter the cells—and also seems to block them from replicating once they are already inside.
But, she added: "While it worked in vitro, I am still waiting to see published results of large blind clinical trials demonstrating the efficacy of HCQ in vivo," she told AFP.
The case for caution
Promise doesn't mean proof, and the small studies carried out so far amount to "anecdotal" evidence, according to Anthony Fauci, head of infectious diseases at the US National Institutes of Health.
What's more, a small Chinese study on 30 patients that was also published this month found HCQ was no better than standard care—meaning treating the symptoms via bed rest, fluids and so on—adding a note of caution to the discourse.
The only way to know for sure is to carry out randomized clinical trials, scientists say. Such experiments are considered the gold standard in the field but last months or years and involve thousands of patients, often from around the world.
Patients are assigned at random to either receive the drug under investigation or a placebo, and the studies are "blinded" meaning the participants and their doctors are unaware which group they are in, to further reduce bias.
Overhyping medicine can have several unintended effects, warn experts.
The small studies carried out so far amount to "anecdotal" evidence, said Anthony Fauci, head of infectious diseases at the US National Institutes of Health - here with President Donald Trump
"One of the unintended consequences are drug shortages of chloroquine, for people that need to manage their rheumatoid arthritis, for example," Peter Pitts, a former commissioner of the Food and Drug Administration told AFP.
A few countries are taking a cautious approach. Spain, for example, announced Monday said that "until further notice" these arthritis and lupus patients would be given priority access to the drug.
French Health Minister Olivier Veran meanwhile said the compounds can be used only to treat the most severe cases of COVID-19.
Another problem is that people may try to self-medicate. A US man from Arizona died this week after ingesting a form of chloroquine intended to fight aquatic parasites.
Side effects
Several countries have now embarked on clinical trials, including the United States, where one began in New York this week.
Italy is carrying out a trial on 2,000 people, while scientists are also awaiting the results from bigger trials in China.
But while the drugs are being rolled out for compassionate use, it is critical to bear in mind safety precautions.
About one percent of people are at high risk of blackouts, seizure or even sudden death from cardiac arrest because of heart rhythm issues they may themselves be unaware of, Michael Ackerman, a genetic cardiologist at Mayo Clinic told AFP.
Medical teams must therefore perform electrocardiograms to inform their risk analysis before using these medicines, he said.
"All focus is placed on the hope for therapeutic efficacy of these medications, without any reasonable amount of respect, not fear, but respect for what the potential side effects of these very powerful medications are," said Ackerman.
2020 AFP
The risks of using 3-D printing to make personal protective equipment
"The production of PPE, for example masks, is much more complicated than people might appreciate, and 3D printed masks may do more harm than good," says Professor Martin Culpepper. Seen here, a surgeon wears a protective mask. Credit: Massachusetts Institute of Technology
As the number of hospitalizations due to COVID-19 continues to rise across the U.S., addressing the shortage of personal protective equipment (PPE) for health care workers has become increasingly urgent. Institutions and organizations across the country—including MIT—have been scrambling to collect and send unused face masks to local hospitals.
28 mar 2020--In the race to help protect doctors, nurses, and patients, some have suggested that technologies like 3-Dprintingbe used to quickly manufacture masks. In a recent memo, MIT faculty members Martin Culpepper, Peter Fisher, and Elazer Edelman, with input from Neil Gershenfeld and A. John Hart, detail the risks associated with using 3-D printing to build PPE and COVID-19-related medical devices.
Martin Culpepper is a professor of mechanical engineering, director of Project Manus, and a member of MIT's governance team on manufacturing opportunities for COVID-19. Here, he discusses the risks associated with using 3-D printing for PPE and what designers, researchers, and engineers can do to address the PPE shortage.
Q: What are the risks associated with using 3-D printing to make PPE for medical professionals?
A: One of the biggest risks with 3-D printing for COVID-19 situations is the false sense of hope that we can quickly print PPE to address needs. Well-intentioned people want to help and think 3-D printing can address the current demand for medical devices and PPE in hospitals. However, the production of PPE, for example masks, is much more complicated than people might appreciate and 3-D printed masks may do more harm than good.
There are a lot of issues with certain types of 3-D printed parts with respect to their use in a clinical setting. One example involves sterilization—material compatibility with the sterilization techniques hospitals currently use and the use of certain materials in a setting where it is uncertain how they interact with other chemicals, devices, and contact with patients and care providers. The thing is though, right now the problem isn't masks, it's the filter media. In particular, the use of filter media in masks is essential to their efficacy.
The filter media is really an amazing thing; it just looks like a simple piece of cloth, but it's made through a very specific process to achieve a very specific end state. This end state is specially engineered to catch small particles. Some materials are electrostatically charged so that small particles become stuck to the fibers as they try to go through. This material works great for clinical use and is urgently needed right now. People are focusing on the masks themselves, and not addressing the real problem—filter media for the masks. Masks without the filter media don't make much of a difference in protecting people from the spread of viruses like COVID-19.
Professor Martin Culpepper co-authored a memo on the use of 3D printing for Covid-19 response at MIT. Credit: Len Rubenstein
Q: How should designers and engineers utilize 3-D printing to develop COVID-19-related medical devices and PPE?
A: At MIT, we have some of the best 3-D printing capabilities you can find on the planet. The reality here is that we aren't large volume manufacturers: Our 3-D printing technologies are set up to build proof-of-concept designs, not to manufacture medical products at scale. The best use of our 3-D printing technologies right now is to use them to rapidly demonstrate the feasibility needed to pave the way to high-rate manufacturing processes. Then we can work with manufacturers who can quickly spin the products up and produce these items at the rate that is needed.
The sheer volume of the need is another reason we are discouraging the use of 3-D printing to produce PPE on MIT's campus. Some hospitals need thousands of pieces of PPE each day, 3-D printing just cannot keep up with that demand. However, if you can come up with a great idea for PPE that can be fabricated in a high-rate way that meets demand, then we encourage people to use 3-D printing as a means to prototype. Once you have that 3-D printed proof of concept prototype, MIT can look to have it rapidly vetted for use in a clinical setting and find manufacturers and medical device companies who are equipped to build and distribute products at scale.
Q: Where should researchers and engineers be focusing their efforts to help solve the PPE shortage?
A: The fastest and safest way to make an impact is to donate unopened PPE that is marketed with regulatory approval. For members of the MIT community, use the MIT program. For people elsewhere, don't take it to a local hospital—instead find an official that is coordinating a local effort and contact them. The second most important thing is fostering collaborations and connections with others.
At MIT, we are working on a few realistic PPE designs that are suitable for rapid deployment to high-rate manufacturing processes. These prototypes are being vetted for deployment. There are many in the community that are supporting each other by offering design advice, sourcing advice, clinical feedback through MIT's connections, and helping find places where they can connect with manufacturers if appropriate.
MIT has always been a place where great ideas can make a big difference in the world. If we are going to make a big difference in this crisis, now is the time for great ideas. One of our strengths at MIT is that we focus on "mind, hand, and heart." This is a time when we need to use all three of those things. People across the world are worried and uncertain. Too many people are "throwing spaghetti at the wall" to see what sticks and not thinking things through. We can only solve these problems in the fastest, smartest way if we continue to apply the motto of "mind, hand, heart" to our efforts.
John Yost and Joshua Kim model the first and second prototypes of the 3D printed masks created by a multidisciplinary team at MUSC. Credit: Sarah Pack
With the threat of a shortage of protective masks looming as the novel coronavirus pandemic grows, Medical University of South Carolina (MUSC) biomedical engineers and tinkerers had an inspired idea: unleash an army of makers from across the U.S. who could make such masks from 3-D printers—a technology that, in recent years, has become widely available.
28 mar 2020--"High schools have a printer capable of making this," said Michael Yost, Ph.D., vice chair of research in the Department of Surgery. "Let's make this so simple that a high schooler could do it, yet effective to protect our people."
In a matter of days, a team came together and developed the Self-Assembly Filter for Emergencies, or SAFE, Cartridge System. The system could be used by medical professionals or by people who just need to go to the grocery store.
The team has been in contact with the U.S. Food and Drug Administration to obtain emergency approval of the device. For now, the device remains investigational and should not be used as a replacement for conventional and approved Personal Protective Equipment.
Yost said the team is talking to manufacturers to see if the design can be mass produced once it has received approval.
The N95 masks that are currently in such short supply are essentially filters molded into mask form. Recreating those masks exactly proved too difficult. So instead, the team created a two-part solution: a 3-D printed mask that can be cleaned and reused that will work in tandem with a 3-D printed disposable filter cartridge. Alternatively, the filter cartridge could be used with an adapted hospital mask.
Joshua Kim, senior designer and program coordinator in the Department of Surgery Human-Centered Design Program, said he was inspired by the NASA engineers during the Apollo 13 disaster, who quickly devised a makeshift carbon dioxide removal system from materials on hand inside the lunar module, including duct tape and plastic.
"How can we utilize materials that people can get at a local hardware store and repurpose those materials to make protective equipment?" he asked.
The "95" in N95 means these masks filter 95% of particulates of a certain size, he explained. HEPA filters, like those used in air purifiers, filter around 99% of particulates. So he bought a HEPA filter and set about experimenting. Using the same testing that's used on N95 masks, he found that using those filters in the homemade cartridge did work—a positive sign that they were on the right track.
Meanwhile, another group was working on creating the masks. Dentists Walter Renne, D.M.D., and Christian Brenes Vega, D.D.S., regularly use 3-D printing. "It's just a part of the job," said Renne, who estimated that 20% of dentists and 90% of dental labs have a 3-D printer on hand. They enlisted the help of John Yost, a student and independent contractor who serves as a resource for all things associated with 3-D printing on campus.
Joshua Kim of Medical University of South Carolina shows how the filter cartridge can be adapted to fit onto existing masks. Credit: Sarah Pack, Medical University of South Carolina
A team at MUSC developed a DIY protective mask that anyone with a 3-D printer can copy.
Initially, they developed different prototypes that would work with different types of filters, including filters used by painters or people dealing with asbestos. They 3-D scanned a mask to get the basic shape, then designed modifications so the mask could accommodate the disposable filter cartridge. The filter, noted Brenes Vega, is the most important part. Unfortunately, some people have turned to masks that aren't actually offering protection, he said.
Finally, they needed to solve the problem of releasing air pressure, Kim said. The filters are so effective that when the wearer exhales, the air will go to the area of least resistance to escape—in other words, not through the filter again but by causing the mask to lift slightly off the wearer's face. That exposes the wearer to the outside air and renders the mask worthless, Renne said. In response, the team installed a rubber valve, commonly used in other medical applications, that allows the exhaled air to escape the mask. As soon as the wearer inhales, the valve immediately shuts, Kim said, protecting the wearer.
Kim said that, for additional sealing and comfort, they added strips of neoprene weatherstripping foam around the edges of the mask. The foam provides a comfortable fit so the wearer's skin isn't touching the plastic mask and ensures it contours to the face as the wearer moves or talks.
With all the parts in place—the 3-D printed mask and 3-D printed cartridge fitted with a hand-cut HEPA filter and rubber valve—the group began fit-testing.
They took four prototypes to the Emergency Department and tested them on several users. So far, the masks have fit everyone, Yost said, although they want to expand their testing to include more face sizes and shapes.
The team is already printing masks at MUSC, even as they continue to perfect the design.
The biggest obstacle now is the time it takes to create the masks. MUSC's 3-D printers aren't production-level printers. They're meant for creating prototypes when time isn't of the essence. It takes about four to five hours to print a mask and then about an hour to assemble everything.
Because of that time element, Yost is talking to manufacturers who could produce these in greater numbers. But the team is also openly releasing the plans so that anyone with a 3-D printer can produce the masks.
In addition to creating the entire mask, makers could create just the disposable cartridge, which can be adapted to fit into the masks used in anesthesiology to deliver oxygen to patients.
Coronavirus might cause loss of smell—but it probably won't be permanent
by Jenny Ekberg, Heidi Walkden and James St John, The Conversation
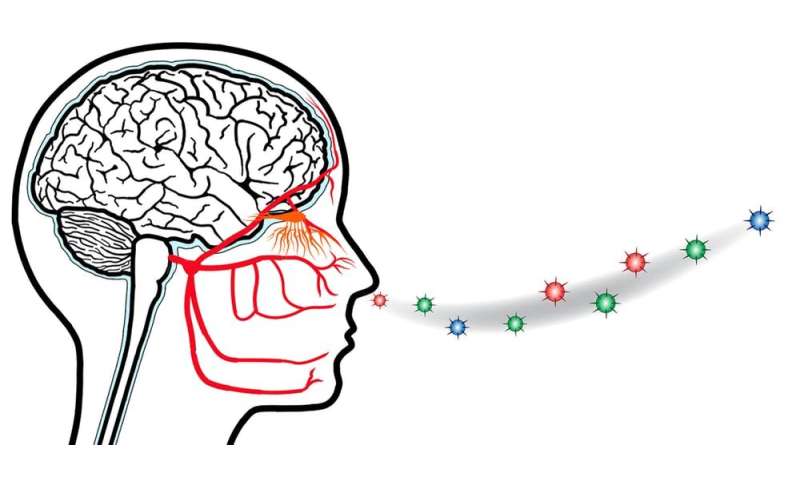
In humans, it has been shown that some types of human coronaviruses can enter the brain from the olfactory bulb at the end of the olfactory nerve. To date, it remains unknown whether SARS-CoV-2 can damage the olfactory nerve. Credit: James St John, Author provided
Reports from South Korea, China and Italy say losing the sense of smell and taste may be a symptom of COVID-19, the disease caused by the coronavirus SARS-CoV-2. Specialists in the UK have suggested the loss of smell, also called anosmia, could even be an early indication of infection.
28 mar 2020--While the exact details of what happens with this coronavirus are unclear, evidence from other infections suggests that while damage to the sense of smell is possible, it's unlikely to be permanent.
Can viruses get into your nerves?
Viruses and bacteria are constantly bombarding the lining of the nose. Luckily our defence mechanisms prevent most pathogens penetrating into the deeper layers of tissue.
Yet some pathogens can penetrate the nasal lining and are known to enter the olfactory nerve, which is responsible for the sense of smell. Pathogens can also enter the trigeminal nerve, which is responsible for controlling biting and chewing, and for sensation in the face.
If viruses or bacteria do enter the nerves, the consequences can be serious. Perhaps the most striking example is Bell's palsy, where part of the face is temporarily paralyzed, and which may sometimes be caused by viral infection of the facial nerve.
Do other viruses affect the sense of smell?
Other viruses, including influenza and herpes, are known to infect the olfactory nerve. From animal studies using other types of coronaviruses (not SARS-CoV-2, the virus that causes COVID-19) we also know that a nasal inoculation with mouse hepatitis virus, which is a type of coronavirus, can rapidly penetrate the olfactory nerve and then continue up into the brain.
In humans, it has been shown that some types of human coronaviruses can enter the brain from the olfactory bulb at the end of the olfactory nerve. To date, it remains unknown whether SARS-CoV-2 can damage the olfactory nerve.
Bacteria also penetrate the olfactory nerve. Our research team has shown that Burkholderia pseudomallei, which causes the tropical disease melioidosis, can kill the olfactory nerve cells and then enter the remnants of the olfactory nerve to move up into the brain.
Once pathogens are inside the olfactory nerve, it is like a highway from the nose to the brain. If the infection kills off nerve cells, it's even easier for the pathogens to move along the nerve.
How does an infection affect the sense of smell?
This killing of the olfactory nerve cells is likely to be the main reason people lose their sense of smell after an infection. Once 20-30% of the olfactory nerve cells have died, people will report they have lost their sense of smell.
If a person has lost 30% of their olfactory nerve cells, they won't be able to detect enough odour molecules to activate the threshold level for smelling when they breathe normally. However, if they sniff harder they will probably be able to smell enough to recognize an odor.
Our research with bacteria has shown that olfactory nerve damage can occur within 24 hours of initial exposure, and (unpublished) results with other viruses show they can act even more quickly. In this way, loss of sense of smell can indeed be an early indicator of a potential pathogen onslaught within the nasal system.
Why is taste affected as well?
What we usually think of as "taste" when we enjoy a delicious meal is actually the combination of smell and taste. When people lose their sense of smell, the major contribution to the enjoyment of food is lost.
This is why people may report they have also lost their sense of taste—which strictly speaking depends on the tongue and taste buds—when they have lost only their sense of smell.
Why do only some people with COVID-19 lose their smell?
Our bodies and immune systems are very diverse, due to genetics and circumstances. Not all people will be susceptible to particular pathogens or affected in the same way.
Our research in mice has clearly demonstrated not only that different strains of mice are susceptible to different bacteria but also that different nerve routes can be affected.
While we do not yet know if SARS-CoV-2 does harm the olfactory nerve, a similar process could explain why some people report a loss of smell and some don't.
Will it be permanent?
Luckily, the olfactory system is designed to survive the constant bombardment of pathogens so if you do lose your sense of smell it will only be temporary. While the olfactory nerve cells that are present within the nasal lining can be infected and die off, stem cells that lie beneath the nerve cells rapidly generate new nerve cells to replace the lost ones.
The new nerve cells grow their long connections back up into the brain to restore the pathway. Depending on the severity of the initial infection, the sense of smell can return within a few days or weeks.
Provided by The Conversation
Coronavirus survives on surfaces: Tips for handling money, food and more
Like the other 200 or so respiratory viruses we know of, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the new coronavirus, infects the cells of our airways.
28 mar 2020--It causes a range of signs and symptoms, or none at all. It can spread easily from person-to-person, and can be coughed into the air and onto surfaces.
Viruses only replicate inside a living cell—outside the cell, they're on a path to either infect us, or their own destruction. How long a virus survives outside a cell varies.
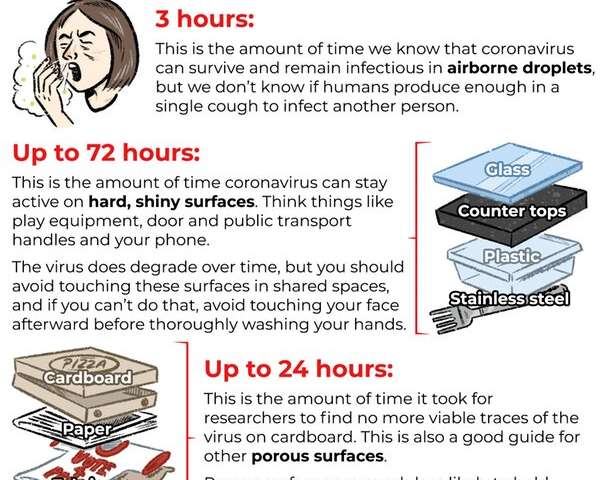
Researchers found SARS-CoV-2 remains infectious in airborne droplets for at least three hours. This doesn't mean infected humans produce enough virus in a cough to infect another person, but they might.
We think the virus also spreads by touch. Hard, shiny surfaces such as plastic, stainless steel, benchtops, and likely glass can support infectious virus, expelled in droplets, for up to 72 hours. But the virus rapidly degrades during this time. On fibrous and absorbent surfaces such as cardboard, paper, fabric and hessian, it becomes inactive more quickly.
How can we reduce risk from surfaces and objects?
Frequently touched surfaces are all around us. Benches, handrails, door handles—they are in our homes, on our way to work, school, play, shop, and every other destination. There's a risk of contaminating these surfaces if we touch them with virus-laden fingers, and a risk we'll contract the virus from such surfaces.
Think of your hands as the enemy. Wash them well, and much more often than usual. Between hand-washing, avoid constantly touching the mucous membranes that lead to your airways. Basically, try not to rub your eyes, pick your nose, or touch your lips and mouth.
Taking precautions through small actions
We're already seeing engineering initiatives to help combat the virus's spread. In Sydney, pedestrian crossings have been automated so people can avoid touching the buttons.
To slow the spread of SARS-CoV-2, assume everything outside your home is potentially contaminated, and act accordingly. So don't touch your face, sanitise frequently while you are out, and wash your hands and clean your phone once home.
While it's best to stay home, keep these tips in mind if you must leave the house.
Going shopping
Grocery shopping requires touching surfaces and items, including trolleys and baskets. Sometimes sanitiser or antibacterial wipes are available for hands and handles at the store entrance—but they're often not, so bring your own (if you can get some). It probably doesn't matter what type of bag you use, but have a plan for how to avoid bringing the virus into your home.
Making payments
Cards and cash could transfer the virus to your hands. That said, card payment is probably lower risk because you retain the card and don't have to touch other people. But wherever possible, contact-free bank transfers would pose the least risk.
Handling and eating fresh and canned food
SARS-CoV-2 is inactivated at temperatures well below those required in the process of canning food, so canned food is free of it. For freshly packaged food, risk depends on whether the person doing the packing was sick or not. If you are concerned, stick with food that can be cooked, peeled or washed in mild soapy water, and thoroughly rinsed.
While evidence is weak, we know soap and water should inactivate SARS-CoV-2 on food—but this will work better on foods with a shinier, harder outer surface, compared to foods that have been cut or have softer surfaces, such as strawberries and raspberries. If you decide to wash any food with soap, make sure all the soap is removed.
At the park
Avoid equipment that is likely used a lot, including play equipment and water fountains. It would be safer to kick a ball around or play on the grass, rather than use swings. Sandpits hold horrors other than SARS-CoV-2.
Takeaway and deliveries
When getting takeaway food, or for businesses offering it, avoid plastic containers and use more fibrous materials such as cardboard, paper and fabric for packaging. Researchers found no infectious SARS-CoV-2 on cardboard after 24 hours.
Also, avoid proximity to servers and delivery people, and opt for contactless delivery whenever you can.
Public transport, escalators, elevators and bathrooms
Frequently touched hard, shiny surfaces such as lift buttons and handle bars in trams are a big risk, more so than fabric seats, or taking the stairs. Even the most high-tech overseas surface cleaning efforts are intermittent, so you'll need to take responsibility for yourself. Also, after using public bathrooms, wash your hands well.
Calm and calculated
It's important to be calm, realistic and not focus on single events or actions once you step outside. You can't account for everything.
Think more about the risk of the entire task rather than the many small risks encountered during the process. A silver lining in taking such precautions is that you'll also reduce your risk of catching the flu this season.
It's also important to keep your home clean. You can use diluted bleach, detergents or alcohol solutions on surfaces. Queensland Health has more information.
Ultimately, the best ways to avoid SARS-CoV-2 infection are primitive ones—sanitise your hands and stay away from others. Physical distancing remains the most effective measure to slow the progression of this pandemic.