Researchers from Western Sydney University's MARCS Institute for Brain, Behavior and Development have published a new research paper and recommended guidelines for music use for people with dementia after a successful trial program.
28 september 2020--Coinciding with National Dementia Action Week, lead researcher Dr. Sandra Garrido and team have this week published their findings and recommendations in a new paper titled: "Music Playlists for People with Dementia: Trialing A Guide for Caregivers" in theJournal of Alzheimer's DiseaseVolume (77) Issue (1).
The trial program, funded by the National Health and Medical Research Council of Australia, was developed to look at the effect of music on people with dementia in aged care facilities and home based care to help manage their symptoms, and investigate how music can be utilized in standardized, yet individually tailored, ways.
Dr. Sandra Garrido launched the trial program after hearing reports that some people were having negative responses, or perhaps not responding to music at all, which lead the team to investigate how people's individual symptoms might be interacting with different types of music.
"We wanted to dig deeper to find out more about how individual symptoms might be interacting with different features of music—such as the tempo, or the lyrics, or the mode—so that we could develop a standardized way that music could be used for people with dementia," said Dr. Garrido.
"Music can have really positive effects, but it's important that its used in standardized ways and that it becomes part of standard care practices in aged care facilities," she said.
The program assists carers and families of people with dementia to use and select music effectively by helping them to identify individuals who might be vulnerable to negative responses to music, and identify particular challenges to care that they may be coping with.
"We teach carers and families how to strategically select music that will specifically help them with their individual symptoms and challenges to care, and help caregivers to identify the particular challenges to care and how to use music to help manage them," explains Dr. Garrido.
"Music is something that we all use in everyday life, and aged care facilities typically have some music going for their residents, however music has the potential to offer so much more than just entertainment for people with dementia."
The recommendations within the new research informed guidelines outline how music can be used as a first line treatment to help deal with some of the psychological and behavioral symptoms of dementia that caregivers are struggling to manage every day.
"Of course, we're not recommending that people don't use pharmaceutical medications when necessary, but there is the potential for music to be used in ways that can cut down on the use of psychotropic and anxiolytic medications, for example, to help cope with some of the symptoms of dementia," said Dr. Garrido.
The guidelines were developed based on scientific research conducted at the MARCS Institute for Brain, Behavior and Development in consultation with people with dementia themselves, their care givers, and care staff in aged care facilities.
Music and filmmaking can transform undergraduate student perceptions of dementia
More information: Sandra Garrido et al. Music Playlists for People with Dementia: Trialing A Guide for Caregivers, Journal of Alzheimer's Disease (2020). DOI: 10.3233/JAD-200457
Journal information: Journal of Alzheimer's Disease
Immunohistochemistry for alpha-synuclein showing positive staining (brown) of an intraneural Lewy-body in the Substantia nigra in Parkinson's disease. Credit: Wikipedia
Although the name may suggest otherwise, Parkinson's disease is not one but two diseases, starting either in the brain or in the intestines. Which explains why patients with Parkinson's describe widely differing symptoms, and points towards personalized medicine as the way forward for people with Parkinson's disease.
22 september 2020--This is the conclusion of a study which has just been published in the leading neurology journalBrain.
The researchers behind the study are Professor Per Borghammer and Medical Doctor Jacob Horsager from the Department of Clinical Medicine at Aarhus University and Aarhus University Hospital, Denmark.
"With the help of advanced scanning techniques, we've shown that Parkinson's disease can be divided into two variants, which start in different places in the body. For some patients, the disease starts in the intestines and spreads from there to the brain through neural connections. For others, the disease starts in the brain and spreads to the intestines and other organs such as the heart," explains Per Borghammer.
He also points out that the discovery could be very significant for the treatment of Parkinson's disease in the future, as this ought to be based on the individual patient's disease pattern.
Parkinson's disease is characterized by slow deterioration of the brain due to accumulated alpha-synuclein, a protein that damages nerve cells. This leads to the slow, stiff movements which many people associate with the disease.
In the study, the researchers have used advanced PET and MRI imaging techniques to examine people with Parkinson's disease. People who have not yet been diagnosed but have a high risk of developing the disease are also included in the study. People diagnosed with REM sleep behavior syndrome have an increased risk of developing Parkinson's disease.
The study showed that some patients had damage to the brain's dopamine system before damage in the intestines and heart occurred. In other patients, scans revealed damage to the nervous systems of the intestines and heart before the damage in the brain's dopamine system was visible.
This knowledge is important and it challenges the understanding of Parkinson's disease that has been prevalent until now, says Per Borghammer.
"Until now, many people have viewed the disease as relatively homogeneous and defined it based on the classical movement disorders. But at the same time, we've been puzzled about why there was such a big difference between patient symptoms. With this new knowledge, the different symptoms make more sense and this is also the perspective in which future research should be viewed," he says.
The researchers refer to the two types of Parkinson's disease as body-first and brain-first. In the case of body-first, it may be particularly interesting to study the composition of bacteria in the intestines known as the microbiota.
"It has long since been demonstrated that Parkinson's patients have a different microbiome in the intestines than healthy people, without us truly understanding the significance of this. Now that we're able to identify the two types of Parkinson's disease, we can examine the risk factors and possible genetic factors that may be different for the two types. The next step is to examine whether, for example, body-first Parkinson's disease can be treated by treating the intestines with feces transplantation or in other ways that affect the microbiome," says Per Borghammer.
"The discovery of brain-first Parkinson's is a bigger challenge. This variant of the disease is probably relatively symptom-free until the movement disorder symptoms appear and the patient is diagnosed with Parkinson's. By then the patient has already lost more than half of the dopamine system, and it will therefore be more difficult to find patients early enough to be able to slow the disease," says Per Borghammer.
The study from Aarhus University is longitudinal, i.e. the participants are called in again after three and six years so that all of the examinations and scans can be repeated. According to Per Borghammer, this makes the study the most comprehensive ever, and it provides researchers with valuable knowledge and clarification about Parkinson's disease—or diseases.
"Previous studies have indicated that there could be more than one type of Parkinson's, but this has not been demonstrated clearly until this study, which was specifically designed to clarify this question. We now have knowledge that offers hope for better and more targeted treatment of people who are affected by Parkinson's disease in the future," says Per Borghammer.
According to the Danish Parkinson's Disease Association, there are 8,000 people with Parkinson's disease in Denmark and up to eight million diagnosed patients worldwide.
This figure is expected to increase to 15 million in 2050 due to the aging population, as the risk of getting Parkinson's disease increases dramatically the older the population becomes.
More information: Jacob Horsager et al, Brain-first versus body-first Parkinson's disease: a multimodal imaging case-control study, Brain (2020). DOI: 10.1093/brain/awaa238
Provided by Aarhus University
Sunday, September 20, 2020
Older people with early, asymptomatic Alzheimer's at risk of falls
Falls are the leading cause of fatal injuries in older adults, causing more than 800,000 hospitalizations and about 30,000 deaths in the U.S. every year. Some risk factors are well-known—advanced age, problems with vision or balance, muscle weakness—but an under-recognized factor is early Alzheimer's disease. Older people in the earliest stages of Alzheimer's, before cognitive problems arise, are more likely to suffer a fall than people who are not on track to develop dementia.
20 september 2020--Researchers at Washington University School of Medicine in St. Louis have found that, in older people without cognitive problems who experience a fall, the process of neurodegeneration that leads to Alzheimer's dementia already may have begun. The findings, available online in theJournal of Alzheimer's Disease, suggest that older people who have experienced falls should be screened for Alzheimer's and that new strategies may be needed to reduce the risk of falling for people in the disease's early stages.
"In the world of fall research, we generally say that you're at risk of falling if you lose strength and balance," said co-senior author Susan Stark, Ph.D., an associate professor of occupational therapy, of neurology and of social work. "If you lose strength and balance, the recommended treatment is to work on strength and balance. But if someone is falling for another reason, maybe because his or her brain has begun accumulating Alzheimer's-related damage, that person might need a different treatment entirely. We don't yet know what that treatment might be, but we hope we can use this information to come up with new treatment recommendations that will reduce the risk of falls in this population."
In 1987, John C. Morris, MD, then a trainee at Washington University, discovered that older people with Alzheimer's dementia are more than twice as likely to suffer a traumatic fall than people of the same age without dementia. Morris is now the Harvey A. and Dorismae Hacker Friedman Distinguished Professor of Neurology and head of the university's Charles F. and Joanne Knight Alzheimer's Disease Research Center.
Since Morris' discovery more than three decades ago, scientists have learned that the brains of Alzheimer's patients start undergoing changes decades before memory loss and confusion become apparent. First, plaques of amyloid proteins form, then tangles of tau protein. Some brain areas begin to shrink, and communication networks between distant parts of the brain start to decay. Stark and colleagues have shown that the link between Alzheimer's and falling holds true even during the silent phase of the disease: People with so-called preclinical Alzheimer's are at increased risk of falling despite having no apparent cognitive problems.
To better understand why people without cognitive symptoms are at risk of falling, first author Audrey Kelemen, a graduate student in Stark's lab, and colleagues followed 83 people over age 65 for a year. All participants were assessed as cognitively normal by a qualified neurologist at the beginning of the study. Each participant filled out monthly calendars recording any falls and underwent brain scans for amyloid and for signs of atrophy and impaired connectivity.
The researchers discovered that the presence of amyloid in the brain alone did not put people at increased risk of falling but that neurodegeneration did. Participants who fell had smaller hippocampi—brain regions that are devoted to memory and that shrink in Alzheimer's disease. Their somatomotor networks—webs of connections that are involved in receiving sensory inputs and controlling movement—also showed signs of decay. The researchers concluded that falling is most likely to occur in the neurodegeneration phase of preclinical Alzheimer's—the last five years or so before memory loss and confusion arise.
"Since I started working on this project, I've started asking my patients about falls, and I can't tell you how often that has helped me start understanding what is going on with the individual," said co-senior author Beau M. Ances, MD, Ph.D., the Daniel J. Brennan, MD, Professor of Neurology and a professor of radiology and of biomedical engineering. Ances treats patients who have dementia and other neurological conditions on the Washington University Medical Campus.
"When a person's mobility is being diminished, even though the person looks very normal, that could be a sign that something needs further evaluation," Ances said. "It's actually a really important potential marker that should make us say, 'Wait a minute. Let's dive into this more. Are there other things that go along with it?'"
The researchers have begun further experiments to better understand why brain changes in Alzheimer's put people at risk of falling, so they can develop fall-prevention recommendations. In the meantime, simple changes could go a long way toward protecting older people from devastating falls, Stark said.
"You can prevent a lot of falls just by making the environment safer," Stark said. "Simple changes could help and can't hurt: making sure the tub isn't slippery; making sure you can get up easily off the toilet; balance and strength training; reviewing your prescriptions to see if certain medications or combinations of medications are increasing the risk of falling. Until we have specific fall-prevention treatments for people with preclinical Alzheimer's, there are still plenty of things we can do to make people safer."
More information: Audrey Keleman et al, Falls Associate with Neurodegenerative Changes in ATN Framework of Alzheimer's Disease, Journal of Alzheimer's Disease (2020). DOI: 10.3233/JAD-200192
Journal information: Journal of Alzheimer's Disease
Saturday, September 19, 2020
Small study supports donor plasma therapy for severe COVID-19
by E.j. Mundell, Healthday Reporter
Using the donated blood plasma of COVID-19 survivors to treat patients in the throes of severe coronavirus illness has met with some controversy. But a small new study suggests it could have real merit.
19 september 2020--The study of 39 patients with severe COVID-19 who were treated at one New York City hospital found the treatment appeared to bump up survival, researchers said.
Plasma is the component of blood that contains immune system antibodies. So-called "convalescent plasma" from COVID-19 survivors is rich in antibodies against SARS-CoV-2, and it's thought that infusing the plasma into COVID-19 patients might help them battle their illness.
On Aug. 23, the U.S. Food and Drug Administration made the unusual and controversial move of granting emergency approval for the use of convalescent plasma for COVID-19—despite a lack of proof of efficacy from randomized clinical trials.
Those trials are underway, but in the meantime anecdotal evidence has suggested that at the very least, the therapy is safe, one expert said.
"I cannot think of one shred of data that I have seen that would suggest harm," said Dr. Liise-anne Pirofski, chair of biomedical research at the Albert Einstein College of Medicine and Montefiore Medical Center, in New York City.
But does convalescent therapy actually help speed recovery from severe COVID-19?
To help find out, a team led by Dr. Nicole Bouvier, of Mount Sinai Hospital in New York City, tracked outcomes for 39 patients hospitalized with COVID-19. They were all very ill: By the time these patients were given a donor plasma transfusion, 87% required supplemental oxygen to breathe, and 10% were on ventilators.
Outcomes for the 39 transfused patients were compared to those of 156 other COVID-19 patients with similar symptoms and medical histories who had not received the experimental treatment.
Reporting Sept. 15 in the journal Nature Medicine, Bouvier's group concluded that "convalescent plasma is potentially effective against COVID-19."
The researchers found that by day 14 after receiving the plasma therapy, 18% of patients still required oxygen supplementation, compared to 28% of those in the "control" group who hadn't gotten the infusion.
By the end of the study in May, 13% of people who got convalescent plasma had died compared with 24% of those who hadn't, the study authors said.
Still, the study was not a large, randomized clinical trial, Bouvier's group said, so the findings are not definitive. "Additional studies are needed to confirm these findings and draw more definitive conclusions about the efficacy of convalescent plasma transfusion for the treatment of COVID-19 in different populations," the team concluded.
Pirofski agreed. "What I think everybody agrees on is the gaps of knowledge that exist can best be addressed by high-quality trials," she said.
Friday, September 18, 2020
Study shows SARS-CoV-2 jumped between people and mink, providing strong evidence of zoonotic transmission
by European Society of Clinical Microbiology and Infectious Diseases
Credit: CC0 Public Domain
A study investigating SARS-CoV-2 infections across 16 mink farms in the Netherlands, being presented at the ESCMID Conference on Coronavirus Disease (ECCVID, held online from 23-25 September) shows that the virus likely jumped between people and mink and back, providing strong evidence that animal to human (zoonotic) transmission is possible.
18 september 2020--The study is by a group of Dutch veterinary science experts including Dr. Bas Oude Munnink (ErasmusMC), Professor Wim van der Poel (Wageningen University and Research Centre), Professor Arjan Stegeman (Utrecht University) Prof Marion Koopmans (ErasmusMC) and Reina Sikkema (ErasmusMC).
The exact origin of SARS-CoV-2 is still unknown, although various theories have been put forward. Animal experiments have shown that non-human primates, ferrets, hamsters, rabbits and bats can be infected by SARS-CoV-2 as well as cats, dogs, lions and tigers. Recently, multiple outbreaks in mink farms (containing mink of the Neovison vison species) in the Netherlands have demonstrated that mink are also susceptible for SARS-CoV-2.
The authors did an in-depth investigation of outbreaks on 16 mink farms and humans living or working on these farms, using whole genome sequencing to underpin sources of transmission. They describe SARS-CoV-2 infections on 16 farms, with over 720,000 animals. In total, 66 of 97 (67%) persons tested had evidence for SARS-CoV-2 infection, either by PCR or serology. All people tested had a direct link to an infected mink farm.
The authors say: "Due to longitudinal follow up of the first 4 farms, we have strong evidence that at least two people on those farms were infected by minks. Unfortunately, based on our research we cannot make definite conclusions on the direction of most of the infections, so we do not know the total number of people that were infected by minks. We conclude that initially the virus was introduced from humans and has evolved on mink farms, most likely reflecting widespread circulation among mink in the first SARS-CoV-2 mink farms, several weeks prior to detection."
They add: "Genetic analysis of SARS-CoV-2 from the human employees on the farms showed they were the same as those found in mink, and were not identical to those found in unrelated SARS-CoV-2 patients living in the vicinity of farms. Genetic sequences from each of the infected mink farms fell into one of five distinct clusters, showing transmission between different mink farms."
They conclude: "Additional research will be needed to determine the routes of transmission. We conclude that at least some of these employees are very likely to have been infected directly from infected mink and thereby describe the first proven zoonotic transmission of SARS-CoV-2 to humans. Close collaboration between human and animal health departments is essential for early identification and control of SARS-CoV-2 infections."
Johns Hopkins Medicine pain experts have joined the International Association for the Study of Pain (IASP) and collaborators worldwide to make a subtle but important update to the definition of "pain" for the first time in 40 years. With this change, the experts aim to make pain diagnosis and management more inclusive of all people who experience it.
"Pain is not just a sensation or symptom. It is a much more complex condition that is important to acknowledge properly to guide basic science research, patient care and public policy," says Srinivasa Raja, M.B.B.S., professor of anesthesiology and critical care medicine at the Johns Hopkins University School of Medicine and chair of the IASP task force that created the revised description.
According to the researchers, the new pain definition—the first update since 1979—features a key phrase (shown in boldface): "An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage."
The phrase is important, say the researchers, because it includes types of pain not well understood 40 years ago, such as nociplastic—where pain receptors are stimulated without evidence of the cause, such as with fibromyalgia—and neuropathic pain caused by a sensitized or maladaptive nervous system, commonly associated with chronic pain conditions such as persistent pains after surgery, nerve injuries and limb amputations (commonly called "phantom limb pain").
The revised definition also is more inclusive of people who cannot express their pain in words. According to Raja, the previous definition used the word "described," which excludes non-verbal behaviors to indicate pain in animals and certain vulnerable individuals.
"Changing this language enables physicians to adequately account for pain in disempowered and neglected populations such as children, the elderly and people with disabilities," he says.
The updated definition can ultimately have an impact on access to health care, if adopted by insurance providers. A 2016 survey by the U.S. Centers for Disease Control and Prevention estimates that 20.4% of U.S. adults live with chronic pain and approximately 20 million reported that pain limits the ability to accomplish tasks in their work and daily life.
"When pain affects peoples' function, psyche and their social well-being, it needs to be recognized by insurance carriers that dictate who gets care and what aspects of their multidisciplinary care are reimbursed," says Raja.
Overall, the IASP task force says the revised definition has provided a starting point to integrate more evidence-based and holistic pain management into medical and mental health care.
"Pain cannot be simplified to a 0 to 10 scale. Assessments instead need to look at the whole person, accounting for the cognitive, psychological and social factors that are critical to treating pain," says Raja.
Provided by Johns Hopkins University School of Medicine
Sunday, September 13, 2020
Telehealth scales up during the pandemic to offer patient care in the safety of the home
Simulation of a virtual urgent care visit at the Medical University of South Carolina. MUSC Health offered these visits for free to help screen patients with suspected COVID-19. Credit: Sarah Pack, Medical University of South Carolina
Hailed for its ability to erase distance between health care providers in cities and patients in rural areas, telehealth has ironically enabled medical care to continue in a time when we all must keep our distance.
13 september 2020--Across the country,telehealthuse has spiked as providers offer virtual patient visits to ensure medical needs are met while minimizing COVID-19 exposure. Regulatory agencies have loosened some restrictions on telehealth during this crisis, and more and more payers have begun to reimburse for it as they would for any other medical service.
The Medical University of South Carolina, one of only two Telehealth Centers of Excellence nationwide, quickly mounted a four-pronged response to the COVID-19 pandemic that ensured both continuity of care for patients with suspected or confirmed COVID-19 and continued ambulatory, also referred to as outpatient, care for all other patients. The team of telehealth and bioinformatics experts who led the effort documented their approach and its success in a recent article in the Journal of the American Medical Informatics Association.
Early on, MUSC Health and telehealth leaders saw the need for a coordinated response to the pandemic.
"The same realization was coming to the forefront of the minds of the leadership, myself included, in telehealth that this was going to be a big problem," said Dee Ford, M.D., director of the MUSC Telehealth Center of Excellence and lead author on the article. "We needed in our own way to create some kind of response to what we believed to be a pretty significant public health problem. Planning started before we even had a case in the state."
Very quickly, MUSC Health was able to stand up virtual screening of patients with suspected COVID-19 and mobile testing sites across the state, a remote home-monitoring program for patients with less severe COVID-19 and a telesitter program for hospitalized patients that enabled providers to monitor and communicate with patients via an audiovisual monitor, minimizing health care exposure and preserving personal protective equipment.
It was able to do so in part because it had long been building its telehealth and bioinformatics capacity. With generous funding from the state, the MUSC Health Center for Telehealth, in coordination with the South Carolina Telehealth Alliance, has been expanding its telehealth services throughout even the remotest regions of the state.
"The state of South Carolina made an investment in MUSC years ago to develop telehealth programs, which then led to a high state of expertise and readiness to pivot when COVID-19 arrived," said Patrick J. Cawley, M.D., CEO of MUSC Health. "The MUSC Health Center for Telehealth is to be congratulated for this ability to lead during this crisis."
Since 2012, when MUSC Health adopted EPIC, an electronic health record, the MUSC enterprise has continued to recruit bioinformatics researchers, mainly housed in the Biomedical Informatics Center (BMIC) and Information Solutions, to customize EPIC to the health system's needs and to learn how to improve care by analyzing EHR data.
Existing telehealth tools would prove invaluable to the initiative, but they had to be radically reimagined and integrated for the purpose of responding to COVID-19. Realizing that the scale of the effort would require easy-to-use options, telehealth leaders also onboarded some new tools, such as the user-friendly telemedicine platform doxy.me, created by BMIC researcher Brandon Welch, Ph.D.
"We had a battlefield-type mentality that we had to all get together to form a new structure," said James McElligott, M.D., executive medical director of the MUSC Health Center for Telehealth.
As they worked to build a unified response and fashion existing tools so as to be COVID-19 relevant, telehealth leaders had the full support of hospital leadership, their colleagues in bioinformatics and the South Carolina Clinical & Translational Research Institute, which provided technical and logistical support.
"No one ever said no, even if that meant working for five months straight and into the late hours of the night and calling up Bioinformatics and saying, 'Make this work like this or change it like this,'" said article co-author Kathryn King, M.D., co-director of the MUSC Telehealth Center of Excellence. "No one ever said no because I think we just knew that it had to happen."
MUSC Health chief research information officer and BMIC director Leslie Lenert, M.D., who is senior author of the article, is proud of his bioinformatics team, which put research aside for a time to help meet this urgent clinical need.
"We took the research capacity we had for EPIC support and improvement, and we told them to stop, and we put them on this full time. That's why we were able to respond so fast," said Lenert. "So we took our best people, and we put them on this problem immediately. We protected their time, and we told them to get something done. We started early, we committed absolutely and we worked with our clinicians to solve practical problems that they had."
With BMIC's help and SCTR's support, existing tools were quickly revamped to ensure continuity of care for patients with suspected or confirmed COVID-19 and continued ambulatory care for all other patients.
Virtual urgent care
Virtual urgent care technology, meant to provide patients a convenient way to be seen for minor illnesses, had to be adapted into a platform for screening patients with suspected COVID-19 and scheduling appointments for them at mobile testing sites throughout the state. Previously, patients reporting serious symptoms, such as shortness of breath, would have been kicked out of that system; therefore, Edward O'Bryan, M.D., telemedicine director for the Emergency Department and direct-to-consumer and institutional telehealth at MUSC, along with other telehealth leaders, had to work rapidly with the virtual urgent care vendor to adapt the technology to screen for COVID-19 symptoms. At the same time, they had to begin staffing up to meet the anticipated demand, increasing the number of providers dedicated to virtual urgent care from fewer than ten to more than a hundred. O'Bryan estimates that more than 150,000 patients have now been screened for COVID-19 through the modified virtual urgent care program.
"We were the first people in South Carolina to offer free virtual care COVID screenings," said O'Bryan. "I'm really proud that we were able to roll it out so quickly and that so many South Carolinians took advantage of it."
BMIC researchers developed an artificial intelligence algorithm that could analyze symptom data provided by patients during virtual urgent care screenings and prioritize those most likely to have COVID-19 for testing. The algorithm proved critical when testing capacity was challenged and should continue to play a key role with the implementation nationwide of "batch testing." Essentially, samples from patients thought to be at low risk of having COVID-19 could be tested in batches of five to extend testing capacity. If the test comes back negative, all five patients are presumed to have a negative result. The algorithm helps identify low-risk patients appropriate for such batch testing while reserving individual testing for higher-risk patients.
"What we were able to do is make a very functional system, which, on the outside, might seem simple -you fill out a questionnaire on a telehealth platform, it goes in and everything happens behind the scenes," said McElligott. "But all of that had to be protected for the patient and linked in with the medical record and the lab. We had to know what to do to get testing sites set up with tents and then use the platforms to guide people there. There's just a whole lot of stuff that had to happen to be able to do this: not one patient at a time, but thousands at a time. We couldn't have done it without the Bioinformatics group stepping in and helping to connect all the dots and then bringing new ideas to the table about how to monitor patients."
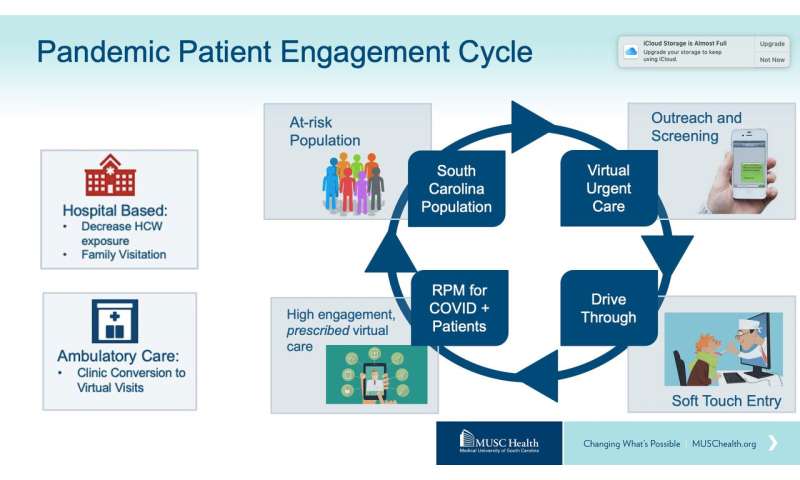
Illustration showing MUSC Health's four-pronged Telehealth response to COVID-19. Credit: MUSC Health Center for Telehealth, Medical University of South Carolina
Remote patient monitoring
In the second prong of the four-pronged approach, patients who tested positive were then invited to enroll in a remote patient monitoring (RPM) program. That program, which had been used to track data on patients with chronic disease, was transformed into a virtual means of monitoring and delivering acute care to patients with less severe COVID-19 who were recovering at home. RPM nurses contacted patients by telephone or text to ask if they wished to enroll in the program. Enrolled patients were asked to answer online survey questions daily about the symptoms they were experiencing and to provide temperature and oxygen saturation values. BMIC researchers created a "best practice alert," which notified a patient's RPM nurse should his or her condition begin to deteriorate. The nurse could then call the patient, alert the patient's primary care provider or arrange for a video consultation with a physician at MUSC Health. Patients who developed more severe disease could be hospitalized.
By the end of August, 735 patients had been treated through the RPM program. Of those patients, 20% were considered high risk and 32% medium risk. Some of these patients lived alone or in rural areas, and the daily contact and calls with RPM nurses were an emotional, as well as a medical, lifeline.
"The lead nurse ends up being a connection to care for a pretty decent number of people who are otherwise fairly isolated," said Ford. "They may live in rural areas. They may be elderly and live alone. They're also supposed to be in quarantine, so they're not supposed to be out and about and have people around them. So, it ends up being an important kind of emotional support tool for folks with cases of COVID-19 that are on home quarantine."
Telesitter program
The third prong of the approach, a telesitter program, is intended for patients hospitalized with more severe disease. An audiovisual cart, previously used to monitor patients to keep them from falling, was adapted so that caregivers could monitor and interact with patients with COVID-19 without having to don and doff personal protective gear each time, at the same time limiting the exposure of the health care worker.
"That's been a real satisfier for the clinical teams. They are able to have that kind of ease of communication without having to go into the patient's room each time," said Ford.
Reimagining outpatient care
In addition to ensuring a smooth continuum of care for patients with COVID-19, the team of telehealth and bioinformatics experts also wanted to provide a way for providers to continue to treat all of their patients, not just those with COVID-19. During the lockdown, most in-person outpatient visits were canceled, leaving many patients without needed medical care. Leaders at the Center for Telehealth quickly began preparing to transition most outpatient visits to telehealth visits -a gargantuan task.
"The scale of response was ... it was something I never thought I'd see," said McElligott.
Article co-author Jillian Harvey, Ph.D., associate professor in the Department of Healthcare Leadership and Management at MUSC, agrees.
"Telehealth has always been seen as the promising solution for access to the health care system, but its utilization hasn't picked up as quickly as we expected," explained Harvey. "Now, because of COVID, there has been a huge ramping up of telehealth across the country, especially in March, April and May."
During that timeframe, telehealth visits soared from less than 5% to more than 70% of all visits at MUSC Health. Between March and July, almost 30,000 outpatients met with their physicians via secure video teleconferencing. To make that happen so quickly, the Center for Telehealth, which previously had been predominantly focused on providing services externally to patients in remote areas of the state, suddenly had to integrate itself more deeply into clinical practice at MUSC Health.
"We had to replicate the whole design of the health system in a microcosm," said McElligott.
Typically, he explained, the Center for Telehealth would have smoothed out work processes and flows for such an initiative, but due to the public health emergency, there was no time.
"So, we set up an organizational structure to try to get this done, changed video technologies to more user-friendly ones, built a bunch of tip sheets about how to do it, and we just rolled it out and let everybody innovate."
And innovate they did. Physicians in every specialty took those tip sheets and figured out for themselves how to overcome every obstacle so that they could begin seeing patients virtually.
"So, the true heroes in all of this are the front-line providers who took the information and figured out how to do it themselves because they knew they had to or patients weren't going to be seen," said McElligott.
The way forward
Due to the pandemic, many more providers, payers and patients have become aware of what telehealth can offer. How deeply it will remain integrated into health systems will depend, in part, on whether payers continue to reimburse for telehealth visits at a similar rate as for in-person care, as they are now doing during the public health emergency.
"This ambulatory care conversion required an infrastructure rebuild but is probably the initiative with the most lasting impact," said King. "Now that providers and patients know what telehealth can do, I don't think they will ever give it up."
"There's no real going back to a lack of telehealth use," said McElligott. "That has probably been forever changed."
Indeed, McElligott believes that the pandemic has helped to transform how providers and the public view health care.
"Our health care system has always been very focused on a provider-centric view of health care. In other words, you as a patient come to the provider, and that's how we work," explained McElligott. "Just using distance technologies starts to reverse that. This terrible pandemic has forced a reckoning and a realization that, in terms of the long-term goals of improving health, it's really more important to meet the needs of patients where they're at."
More information: Dee Ford et al, Leveraging Health System Telehealth and Informatics Infrastructure to Create a Continuum of Services for COVID-19 Screening, Testing, and Treatment, Journal of the American Medical Informatics Association (2020). DOI: 10.1093/jamia/ocaa157
Journal information: Journal of the American Medical Informatics Association
Provided by Medical University of South Carolina
Saturday, September 05, 2020
Many countries falling behind on global commitments to tackling premature deaths from chronic diseases
Trends in the risk of premature death from the main four NCD groups from 2010 to 2016. Credit: The Lancet
Over the next two weeks, The Lancet will be publishing two reports calling for urgent global action on non-communicable diseases (NCDs).
05 september 2020--The NCD Countdown to 2030 tracks global progress onnon-communicable diseasesagainst commitments to reduce deaths from NCDs by a third by 2030. The report will publish Thursday 3rd September.
On Tuesday 14th September, The Lancet will publish a new Commission urging greater action to combat one of the world's biggest and most neglected health disparities: non-communicable diseases and injuries (NCDI) that kill and disable the poorest billion people, many of them children and young adults—and many of them at dire risk amid the COVID-19 pandemic.
Around the world, the risk of dying prematurely from preventable and largely treatable chronic diseases such as stroke, heart disease, and stomach cancer has declined steadily over the past decade, but death rates from other chronic diseases such as diabetes, lung cancer, colon cancer, and liver cancer are declining too slowly or worsening in many countries.
Many countries are falling short or behind on their commitments to reducing premature mortality from chronic diseases, or non-communicable diseases (NCDs). Among high-income countries, only Denmark, Luxembourg, New Zealand, Norway, Singapore, and South Korea are on track to meet the SDG target for both men and women if they maintain or surpass their recent rates of progress.
These are the findings of the 2nd edition of the NCD Countdown 2030 report, published today in The Lancet, ahead of the Global Week of Action on NCDs next week. The 1st NCD Countdown Report was released in 2018.
NCDs currently kill over 40 million people a year worldwide, making up seven out of ten deaths globally. 17 million of these deaths are of people younger than 70 years old and classed as premature; the great majority (15 million) of these deaths are between 30 and 70 years.
In 2015, world leaders signed up to achieve the United Nations' Sustainable Development Goal 3.4 of a one-third reduction in deaths between 30 and 70 years of age from four key NCDs—cancer, cardiovascular disease, chronic respiratory disease, and diabetes—by the year 2030. The NCD Countdown 2030 report, led by Imperial College London, World Health Organization, and the NCD Alliance, reveals that the global goal to reduce premature mortality from NCDs by one third by 2030 is still achievable but many countries are falling short.
"No country can reach that target by simply addressing a single disease—what is needed is a package of measures, a strong health system, which addresses prevention, early detection and treatment, tailored to the national situation," said Majid Ezzati, Professor of Global Environmental Health at Imperial College London, who led the study.
"Young people must lead the fight against NCDs. An estimated 150 million people will lose their lives too early from a noncommunicable disease over the next decade and right now NCDs are intensifying the impact of COVID-19," said Dr. Bente Mikkelsen, Director of Noncommunicable Diseases, World Health Organization. "We must ensure that all NCDs are addressed in COVID-19 recovery plans so that we can turn this deadly tide. We cannot allow NCDs to become a generational catastrophe, where human potential is wasted, and inequality is exacerbated."
NCDs in the context of the COVID-19 pandemic
People living with many NCDs are being disproportionately affected by COVID-19—they are at a considerably higher risk of suffering severe illness and dying from the disease. At the same time, the ability to reach the UN targets is being challenged by the added impact of the COVID-19 pandemic which is severely disrupting the capacity of national health services to deliver regular screening, diagnosis, treatment and prevention of NCDs.
"COVID-19 has exposed how a failure to invest in effective public health to prevent NCDs and provide health care for people living with NCDs can come back to bite us," said Katie Dain, CEO of the NCD Alliance. "The good news is that all countries can still meet the 2030 targets, with sound policies and smart investments. NCD prevention and treatment can no longer be seen a 'nice to have', it must be considered as part of pandemic preparedness."
In an editorial, The Lancet highlights that: "COVID-19 and NCDs form a dangerous relationship, experienced as a syndemic that is exacerbating social and economic inequalities... COVID-19 is a pandemic that must highlight the high burden that NCDs place on health resources. It should act as a catalyst for governments to implement stricter tobacco, alcohol, and sugar controls, as well as focused investment in improving physical activity and healthy diets. COVID-19 has shown that many of the tools required for fighting a pandemic are also those required to fight NCDs: disease surveillance, a strong civil society, robust public health, clear communication, and equitable access to resilient universal health-care systems... COVID-19 must stimulate far greater political action to overcome inertia around NCDs."
Tracking country progress on SDG 3.4
The UN measure of progress towards the SDG target 3.4 is reducing by one-third the risk of death between 30 and 70 years of age from four major groups of NCDs (cancers, cardiovascular diseases (CVDs), chronic respiratory diseases, and diabetes), termed NCD4. Based on recent (2010-2016) trends, the NCD Countdown 2030 report finds that:
Among high-income countries, only Denmark, Luxembourg, New Zealand, Norway, Singapore, and South Korea are on track to meet this target for both men and women if they maintain or surpass their 2010-16 average rates of decline.
17 countries are already on track to reach the SDG target 3.4 for women: Belarus, Denmark, Iran, Kazakhstan, South Korea, Kuwait, Luxembourg, Latvia, Maldives, Norway, New Zealand, Russian Federation, Singapore, Serbia, Timor-Leste, Ukraine.
And 15 countries are on track for men: Bahrain, Belarus, Czech Republic, Denmark, Finland, Iran, Iceland, Kazakhstan, South Korea, Luxembourg, Maldives, Norway, New Zealand, Singapore, Slovakia.
The risk of dying prematurely from NCD4 is declining rapidly in central and eastern Europe.
However, large countries that showed stagnation or small increases in risk of premature death from these NCDs are Bangladesh (men), Egypt (women), Ghana (men and women), Cote d'Ivoire (men and women), Kenya (men and women), Mexico (men), Sri Lanka (women), Tanzania (men) and the USA (women).
Tracking progress on four major groups of NCDs
Worldwide, deaths from stroke, heart disease and stomach cancer are falling, although overall progress has slowed compared to the previous decade, according to WHO. Deaths from diabetes, lung cancer, colon cancer and liver cancer are stagnating or rising in many countries. The NCD Countdown 2030 report shows that:
The risk of premature death from ischaemic and haemorrhagic stroke, heart disease, chronic lung diseases and stomach cancer declined faster than that of other causes. However, heart disease remains the leading cause of premature death in most countries for men and in about half the countries for women.
In contrast, the risk of premature death from diabetes, colorectal cancer, liver cancer, breast cancer and prostate cancer declined more slowly than other causes, as did lung cancer among women.
For lung cancer in women and colorectal, liver and prostate cancers in men, the risk of premature death increased in more than half of countries.
Policies to accelerate decline in premature mortality
The report notes that although premature death from NCDs is declining in the majority of countries, the pace of change is too slow to achieve SDG target 3.4 in most. The authors used mathematical modelling to assess how many options countries have for accelerating mortality decline.
"To move forward we must learn from those countries that are doing well and replicate their strategies to NCD prevention and healthcare," said Professor Ezzati. "Our analysis shows that every country still has options to achieve SDG target 3.4 but they need to address multiple diseases and have strong health systems."
To that end the report highlights the set of interventions needed to move countries forward:
Tobacco and alcohol control and effective health system interventions, such as a ban on advertising, increasing taxes, plain packaging, public smoking/drinking bans.
Quality primary care—including equitable access to doctors' surgeries and community-based clinics.
Quality referral systems and consistent maintenance of people in care to help patients get the right treatment at the right time.
A range of medicines and techniques available for early diagnosis and treatment—such as increased equitable access to preventative cholesterol-lowering, hypertension and diabetes medicines.
Effective cancer screening and treatment—to diagnose and treat cancers earlier, reducing long-term health impacts and premature deaths.
More information: NCD Countdown 2030: pathways to achieving Sustainable Development Goal target 3.4, The Lancet (2020). DOI: 10.1016/S0140-6736(20)31761-X
Provided by Lancet
Friday, September 04, 2020
Corticosteroids reduce risk of death by 20% in critically ill COVID-19 patients
An inexpensive, widely available class of drug called corticosteroids reduces the risk of death among critically ill COVID-19 patients by 20%, an analysis of seven trials published today in the Journal of the American Medical Association (JAMA) has found.
04 september 2020--The World Health Organization (WHO) announced today it is updating its COVID-19 treatment guidance as a result of the findings.
The meta-analysis of seven international trials, co-ordinated by the WHO and with analyses by researchers from St. Michael's Hospital of Unity Health Toronto and the National Institute for Health Research (NIHR) at the University of Bristol, assessed mortality over a 28-day period after the start of treatment. The review found that treatment of the most severely ill patients—those in an ICU—with dexamethasone or hydrocortisone reduced mortality from 40% to 32%, a relative reduction of 20%.
Corticosteroids are a class of drug that lowers inflammation and reduces immune system activity.
The analysis is the result of collaboration between study teams, guideline developers and journals in response to the global pandemic. This meant results could be shared between research teams and with guideline developers before they were published.
"Even beyond the clear evidence of benefit for an inexpensive and widely available medication, the process of this work—pooling data across seven trials conducted over a period of only three months—highlights the willingness of researchers around the world to share data in a new research model that can bring reliable evidence rapidly to improve the care of patients with COVID-19," says Dr. John Marshall, senior scientist at the Li Ka Shing Knowledge Institute at St Michael's Hospital of Unity Health Toronto, and co-chair of the WHO Working Group on Clinical Characterization and Management.
The team behind the review includes the lead researchers from Brazil, Canada, China, France, Spain, the UK and the U.S.. The work is part of the WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) initiative.
The researchers reviewed data from seven randomized control trials that had recruited 1,703 critically ill patients in total. These trials spanned five continents and included some of the countries hardest hit by COVID-19. They also included critically ill patients from the RECOVERY trial, which reported its findings in June 2020, and patients from the REMAP-CAP trial, the Canadian arm of which was led by Dr. John Marshall of St. Michael's Hospital. Unity Health Toronto's Arthur S. Slutsky, a scientist at St. Michael's Hospital, was also an author on the review paper.\
Data from three of the seven trials in the meta-analysis, including the REMAP-CAP trial, were also published today inJAMA.
The mortality results were consistent across the seven trials with two types of corticosteroid, dexamethasone and hydrocortisone, giving similar effects. Too few patients were included in trials of methylprednisolone to allow its effect to be estimated with precision.
There was evidence of benefit from corticosteroids regardless of whether patients were receiving invasive mechanical ventilation at the time they started treatment. The benefit appeared greater among patients who were not so sick that they needed medicine to support their blood pressure, although the results were not definitive in this regard. The effect of corticosteroids appeared similar regardless of age, sex or how long patients had been ill.
"Our review is good news in the effort to treat COVID-19, and provides important new information that builds on the findings of the RECOVERY trial," says Jonathan Sterne, Professor of Medical Statistics and Epidemiology, University of Bristol and Deputy Director of the NIHR Bristol Biomedical Research Center (NIHR Bristol BRC). "Steroids are a cheap and readily available medication, and our analysis has confirmed that they are effective in reducing deaths amongst the people most severely affected by COVID-19. The results were consistent across the trials and show benefit regardless of age or sex."
Janet Diaz, lead, clinical response for COVID-19, WHO Emergency Program added: "WHO is committed to transforming science to policy in order to save lives. The COVID-19 pandemic has challenged us to work faster, but not to sacrifice quality and standards. The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group demonstrates how, in solidarity, science and public health can come together quickly for a common cause. The milestone of pooling of trial data before publication, using that data to inform clinical guidance development and then simultaneous publication of the evidence, evidence synthesis and guidance is unprecedented. I am privileged to have been part of this tremendous collaboration."
More information: undefined undefined et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19, JAMA (2020). DOI: 10.1001/jama.2020.17023
Journal information: Journal of the American Medical Association

 of an intraneural Lewy-body in the Substantia nigra in Parkinson's disease. Credit: Wikipedia")