AstraZeneca, UK PM defend Covid jab's effectiveness
Credit: Pixabay/CC0 Public Domain
AstraZeneca and British Prime Minister Boris Johnson on Thursday defended the effectiveness of the company's COVID-19 vaccine after regulators in Germany said it should not be given to over-65s.\
28 jan 2021--A spokesperson for the UK-based company said the latest clinical trial data for itsvaccine, developed with Oxford University, "support efficacy in the over 65 years age group".
The company is awaiting a decision from the EU's medicines regulator, the spokesperson added.
Johnson meanwhile told reporters that the UK's own regulator had established "that they think the Oxford/AstraZeneca vaccine is very good and efficacious, gives a high degree of protection".
A panel of scientific experts in Germany said the vaccine should only be used for "persons aged 18 to 65 years old based on available data", citing "insufficient data" to assess its efficacy for older people.
Britain has been using the Oxford/AstraZeneca jab along with another developed by Pfizer/BioNTech across all older age groups as it bids to immunise the most vulnerable 15 million people by mid-February.
Mary Ramsay, head of immunisations at the government agency Public Health England, also backed the AstraZeneca vaccine for older recipients.
"Both the AstraZeneca and Pfizer/BioNTech vaccines are safe and provide high levels of protection against COVID-19, particularly against severe disease," she said.
"There were too few cases in older people in the AstraZeneca trials to observe precise levels of protection in this group, but data on immune responses were very reassuring," Ramsay added.
"The risk of severe disease and death increase exponentially with age—the priority is to vaccinate as many vulnerable people as possible with either vaccine, to protect more people and save more lives.
German draft doesn't recommend AstraZeneca jab for over-65s
A man wears a face mask as he comes back from the vaccination center in Frankfurt, Germany, Thursday, Jan. 28, 2021. (AP Photo/Michael Probst)
A draft recommendation from Germany's vaccination advisory committee calls for offering the AstraZeneca vaccine only to people aged 18-64 for now, citing what it says is insufficient data to judge its effectiveness for older people.
28 jan 2021--The European Medicines Agency is expected to approve the AstraZenecavaccinefor use in the 27-nation European Union on Friday. It would be the third cleared for use in the EU after the BioNTech-Pfizer and Moderna vaccines.
In a draft recommendation released on Thursday ahead of that decision, Germany's permanent vaccination commission called for using AstraZeneca's vaccine for the 18-64 age group on the basis of currently available information. It said that "there currently is not sufficient data to assess the vaccination effectiveness from 65 years."
AstraZeneca noted earlier this week that British regulators supported its use in the older age group despite lack of late-stage effectiveness data. The company pointed to earlier-stage data published in the journal Lancet in November "demonstrating that older adults showed strong immune responses to the vaccine, with 100% of older adults generating spike-specific antibodies after the second dose."
But questions remain about how well the vaccine protects older people. Only 12% of participants in the AstraZeneca research were over 55 and they were enrolled later, so there hasn't been enough time to see whether they get sick at a lower rate than those who didn't get the vaccine.
German Health Minister Jens Spahn stressed that the committee's recommendation isn't its final decision, and that will be made only after the vaccine is cleared for use.
But he said there had been a discussion since autumn about there being "few data—this isn't about bad data, but few data" in studies on the AstraZeneca vaccine's effectiveness in older groups.
"It was to be expected that this would have an influence on the decision of the regulatory authorities and then the permanent vaccine commission," Spahn said. "We just don't know yet how concretely—so let's wait for the decision tomorrow on clearance and then the final recommendation from the permanent vaccine commission."
When Britain approved the AstraZeneca vaccine for emergency use last month, it acknowledged that data regarding its effectiveness in older people was "limited."
The vaccination committee, known by its German acronym STIKO, is an independent expert panel that provides advice to the government and the medical profession on which immunizations should be given to whom. It doesn't play a direct role in the vaccine approval process, but its advice determines what vaccines are considered standard for which groups, and therefore covered by health insurance.
Taking a regular afternoon nap may be linked to better mental agility, suggests research published in the online journal General Psychiatry.
26 jan 2021--It seems to be associated with better locational awareness,verbal fluency, and working memory, the findings indicate.
Longer life expectancy and the associated neurodegenerative changes that accompany it, raise the prospect of dementia, with around 1 in 10 people over the age of 65 affected in the developed world.
As people age, their sleep patterns change, with afternoon naps becoming more frequent. But research published to date hasn't reached any consensus on whether afternoon naps might help to stave off cognitive decline and dementia in older people or whether they might be a symptom of dementia.
The researchers explored this further in 2214 ostensibly healthy people aged at least 60 and resident in several large cities around China, including Beijing, Shanghai, and Xian.
In all, 1534 took a regular afternoon nap, while 680 didn't. All participants underwent a series of health checks and cognitive assessments, including the Mini Mental State Exam (MMSE) to check for dementia.
The average length of night time sleep was around 6.5 hours in both groups.
Afternoon naps were defined as periods of at least five consecutive minutes of sleep, but no more than 2 hours, and taken after lunch. Participants were asked how often they napped during the week; this ranged from once a week to every day.
The dementia screening tests included 30 items that measured several aspects of cognitive ability, and higher function, including visuo-spatial skills, working memory, attention span, problem solving, locational awareness and verbal fluency.
The MMSE cognitive performance scores were significantly higher among the nappers than they were among those who didn't nap. And there were significant differences in locational awareness, verbal fluency, and memory.
This is an observational study, and so can't establish cause. And there was no information on the duration or timing of the naps taken, which may be important.
But there are some possible explanations for the observations found, say the researchers.
One theory is that inflammation is a mediator between mid-day naps and poor health outcomes; inflammatory chemicals have an important role in sleep disorders, note the researchers.
Sleep regulates the body's immune response and napping is thought to be an evolved response to inflammation; people with higher levels of inflammation also nap more often, explain the researchers.
More information: Relationship between afternoon napping and cognitive function in the ageing Chinese population, General Psychiatry, DOI
In the inaugural issue of the journal Nature Aging a research team led by aging expert Linda P. Fried, MD, MPH, dean of Columbia University Mailman School of Public Health, synthesizes converging evidence that the aging-related pathophysiology underpinning the clinical presentation of phenotypic frailty (termed as "physical frailty" here) is a state of lower functioning due to severe dysregulation of the complex dynamics in our bodies that maintains health and resilience. When severity passes a threshold, the clinical syndrome and its phenotype are diagnosable. This paper summarizes the evidence meeting criteria for physical frailty as a product of complex system dysregulation. This clinical syndrome is distinct from the cumulative-deficit-based frailty index of multimorbiditys.
23 jan 2021--Physical frailty is defined as a state of depleted reserves resulting in increased vulnerability to stressors that emerges during aging independently of any specific disease. It is clinically recognizable through the presence of three or more of five key clinical signs and symptoms: weakness, slow walking speed,low physical activity, exhaustion and unintentional weight loss.
The authors of this Perspectives article integrate the scientific evidence of physical frailty as a state, largely independent of chronic diseases, that emerges when the dysregulation of multiple interconnected physiological and biological systems crosses a threshold to critical dysfunction that severely compromises homeostasis, or stability among the body's physiological presses. The physiology underlying frailty is a critically dysregulated complex dynamical system. This conceptual framework implies that interventions such as physical activity that have multisystem effects are more promising to remedy frailty than interventions targeted at replenishing single systems.
Fried and colleagues then consider how this framework can drive future research to optimize understanding, prevention and treatment of frailty, which will likely preserve health and resilience in aging populations.
"We hypothesized that when Individual physiological systems decline in their efficiency and communication between cells and between systems deteriorate, this results in a cacophony of multisystem dysregulation which eventually crosses a severity threshold and precipitates a state of highly diminished function and resilience, physical frailty," said Fried, who is also director of the Robert N. Butler Columbia Aging Center.
"The key insight is simply that one's physiological state results from numerous interacting components at different temporal and spatial scales (e.g., genes, cells, organs) that create a whole unpredictably more than the parts," observes Fried.
For example, Fried notes that physical frailty prevalence and incidence has been linked to the interconnected dynamics of three major systems, alteredenergy metabolismthrough both metabolic systems, including glucose/insulin dynamics, glucose intolerance, insulin resistance, alterations in energy regulatory hormones such as leptin, ghrelin, and adiponectin, and through alterations of musculoskeletal systems function, including efficiency of energy utilization and mitochondrial energy production and mitochondrial copy number. Notably, across these systems, both energy production and utilization are abnormal in those who are physically frail.
The aggregate stress response system and its subsystems are also abnormal in physical frailty. Specifically, inflammation is consistently associated with being frail, including significant associations with elevated inflammatory mediators such as C-reactive protein, Interleukin 6 (IL-6, and white blood cells including macrophages and neutrophils, among others, in a broad pattern of chronic, low-grade inflammation. Each of these three systems mutually regulate and respond to the others in a complex dynamical system.
The authors recommend that multisystem fitness is needed to maintain resilience and prevent physical frailty, including macro-level interventions such as activities to improve physical activity or social engagement; the latter, apart from contributing to psychological well-being, also can increase physical and cognitive activity.
"There is strong evidence that frailty is both prevented and ameliorated by physical activity, with or without a Mediterranean diet or increased protein intake," noted Fried.
"These model interventions to date are nonpharmacologic, behavioral ones, emphasizing the potential for prevention through a complex systems approach."
"This work, conducted under the leadership of Dr. Linda Fried, is the culmination of nearly two decades of research characterizing the pathophysiology of the frailty syndrome. It should pave the way for further elucidating the underlying mechanisms of frailty pathogenesis," said Ravi Varadhan, Ph.D., Ph.D., Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University, and a co-author. "The paper postulates that energetics—the totality of the processes involved in the intake, utilization, and expenditure of energy by the organism—is the key driver of frailty. Testing this hypothesis would be an important area of future research in aging."
More information: Fried, L.P., Cohen, A.A., Xue, QL. et al. The physical frailty syndrome as a transition from homeostatic symphony to cacophony. Nat Aging 1, 36–46 (2021). doi.org/10.1038/s43587-020-00017-z
Provided by Columbia University's Mailman School of Public Health
Wednesday, January 13, 2021
Use of telehealth jumped as pandemic shutdown began
Use of telehealth jumped sharply during the first months of the coronavirus pandemic shutdown, with the approach being used more often for behavioral health services than for medical care, according to a new RAND Corporation study
13 jan 2021--Between mid-March and early May 2020,telehealthwas used by more than 40% of patients with a chronic physical health condition and by more than 50% of those with a behavioral health condition, according to findings published in theJournal of General Internal Medicine.
Overall, almost half of the people who were undergoing treatment when the pandemic shutdown began reported using some form of telemedicine.
Researchers found that the use of telehealth for behavioral health conditions was lower among women and among people over the age of 60. Use of telehealth also was lower among Non-Hispanic Whites relative to Non-Hispanic Blacks, and was lower among those with less than a high school education relative to those with a college degree.
"While the increased use of telehealth was widespread, some groups of Americans reported using the services less often than others," said Dr. Shira H. Fischer, the study's lead author and a physician researcher at RAND, a nonprofit research organization. "If telehealth use is going to remain high, we need to ensure equity of access, particularly for behavioral health care where education, age and gender were all associated with levels of use."
In a finding with important implications for the future of telehealth, researchers also found that during the pandemic a large majority of telehealth users connected with their own doctor rather than a new or unfamiliar doctor.
Prior to the pandemic, patients frequently were reluctant to use telehealth because it often meant seeing a provider other than their own physician. According to researchers, sustaining the ability to see one's own doctor through telehealth may be critical to making telehealth a permanent part of routine health care.
Many reports have documented a spike in the use of telehealth services after the shutdown prompted by the coronavirus pandemic. The increase was made possible by emergency regulatory changes that were adopted to promote use of telehealth.
RAND researchers examined the increase in telehealth by surveying 2,052 adults who are a part of the RAND American Life Panel, a nationally representative internet panel. The questions about use of telehealth were part of a larger survey about life during the pandemic that was fielded between May 1 and May 6.
When the pandemic began, nearly 40% of the Americans surveyed were being treated for a chronic physical health condition, while 15% were being treated for a behavioral health condition. Since the pandemic started, 16% had considered seeking care for a new or recurrent condition.
The study found that among patients who were receiving care when the pandemic began, 11% had used telehealth that included video conferencing from the middle of March to early May, a period of less than two months. In contrast, a survey conducted with the same panel in 2019 found that fewer than 4% had ever used video conferencing with a doctor.
Among people who used telehealth services, researchers found that the use of video telehealth was less common for physical health care (14% of patients) than for behavioral health care (30% of patients).
Lack of insurance was associated with lower telehealth use for new conditions, while use of telehealth was more common in the Northeast than other parts of the nation.
"There is a wide expectation that telehealth will continue after the pandemic ends. Lessons from the use of telehealth during this period should inform policy for the post-COVID-19 era," Fischer said.
Precision health is an approach to wellness that takes into account variability in genes, environment, and lifestyle for each person. And thanks to advancements in technology, it’s here today. Credit: University of Michigan
Precision health is an approach to wellness that takes into account variability in genes, environment, and lifestyle for each person. And thanks to advancements in technology, it's here today. Huge amounts of data are being collected and analyzed to manage our care, with data sources including laboratory tests, biometric sensors, patient records, hospital data, and more. But results can be slow in coming, and the wait between testing and diagnosis can be days or weeks.
12 jan 2021--However, recent breakthrough developments in technologies for real-time genome sequencing, analysis, and diagnosis are poised to deliver a new standard of personalized care.
Imagine a case in which a patient is admitted to a clinic and a simple blood or saliva test is administered. Before the visit is over, a complete diagnosis and personalized treatment plan is available. In another scenario, a surgeon who is seeking to remove a tumor with minimal impact to healthy tissue could confirm decisions through real-time tissue sample analysis. Finally, picture a portable pathogen detector that could alert a user to dangerous exposure during a pandemic or disease outbreak.
The key to making these and other visions real would be a handheld device that provides real-time genomic sequencing and analysis of patient DNA or pathogen DNA or RNA.
Advances in genetic sequencing
It cost nearly $3 billion to sequence the first human genome in 2001. Today, the cost to sequence a whole human genome is under $1000 and expected to reach about $100 soon. In addition, first- and second-generation sequencing systems were large, expensive, and designed for batch operation. Results would become available days or more after samples were taken. But new, lower-cost third-generation sequencing systems now exist, such as the Oxford Nanopore MinION, which can rapidly sequence individual samples and fit in the palm of your hand.
The human genome is made up of over three billion base pairs of DNA. To sequence a genome, the MinION employs small nanopores to divide a collected sample into billions of strands, called "reads."
"The MinION is a great handheld sequencing tool and is capable of rapidly sequencing biological data," says Reetuparna Das, an associate professor in CSE. "It takes the chemical sample, divides the DNA or RNA into strands, and sequences those strands into electrical signals, known as 'squiggles." However, it does not have the compute capability to analyze raw data in the field and quickly produce actionable results."
All that stands between us and real-time diagnosis is a computing system that can analyze the sequenced data and provide treatment and therapy recommendations before the patient even leaves the office.
The computing challenges
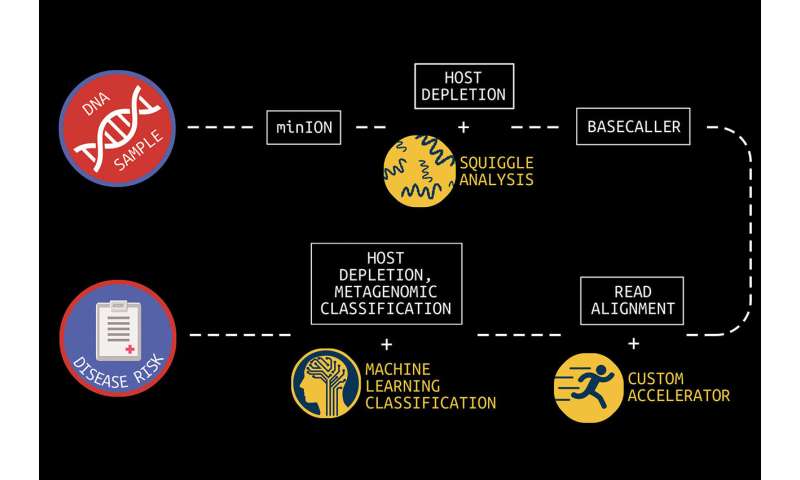
In what is known as secondary analysis, it is the job of a computing system to interpret squiggles as base pairs of DNA, a process which is known as basecalling. A base pair is essentially one rung on a DNA or RNA structure's ladder. Following that, the system must align the read data to genome reference data and then identify variants between the sample and the reference. The variant data of human genomes is used to identify a genetic disease marker. Sequencing is also used to identify pathogens by aligning DNA or RNA strands to a reference pathogen database and using metagenomic classification tools.
U-M researchers are working to bring real-time diagnosis to healthcare providers through combined efforts in computer architecture and machine learning development. This graphic depicts the full pipeline necessary to get from DNA sample to actionable diagnosis. Each step is labeled in a white box, and the tools being developed at U-M to address that step below along with an illustration. The researchers use DNA data sequenced by the Oxford Nanopore MinION device. Credit: University of Michigan
And although this sounds straightforward, sequencing produces about GBs to TBs of data and the processing challenges are steep because of the precision, complexity, and scale of the task. Two multidisciplinary teams of researchers at U-M are working on approaches to overcome this hurdle.
Associate professor Reetuparna Das and professor Satish Narayanasamy, along with professor David Blaauw in Electrical and Computer Engineering, are leading a team funded by the National Science Foundation and the Kahn Foundation that is developing a hardware/software platform to accelerate next-generation genomic sequencing with a focus on pathogen detection and early cancer detection. In this effort, they are collaborating with associate professor of internal medicine and of microbiology and immunology Robert Dickson and assistant professor Carl Koschmann of pediatrics, as well as with associate professor Jenna Wiens, who is also a part of the second research team.
The second team, funded by the Kahn Foundation, is developing data acquisition and machine learning techniques to dramatically improve the prediction, treatment, and management of disease in aging populations. A key component of this effort is the use of machine learning to speed metagenomic analyses.
This large-scale interdisciplinary effort is a collaboration between researchers at Technion—Israel Institute of Technology, the Weizmann Institute, and U-M. The U-M researchers are led by Betsy Foxman, professor of epidemiology at the School of Public Health. Wiens, who is also a Co-Director of U-M Precision Health, is a Co-PI for the U-M research group.
An accelerated computing platform for genomic sequencing
Blaauw, Das, and Narayanasamy are focused on dramatically accelerating and optimizing the pipeline to process data from the MinION. The goal, say the researchers, is to reduce the time required to analyze a sequenced genome from hundreds of CPU hours to a matter of minutes.
"To realize the full potential of genomic sequencing," says Das, "computing power needs to increase by orders of magnitude."
The problem is, that's not possible under traditional processor roadmaps, where additional transistors and cores are packed ever more tightly into a processor for incremental processing gains. Added additional programming cores won't solve the problem either.
"Sustainable growth of processor performance is only possible with custom layers including hardware, software, and algorithms," says Das.
There are a number of areas of inefficiency that occur during secondary analysis which the team is addressing.
First, says Das, is the read alignment process, during which read data is aligned to genome reference data. Read alignment is composed of two steps: seeding and seed extension.
A faster pipeline for analyzing sequenced data: An Oxford Nanopore MinION in the researchers' lab enables rapid, mobile genome sequencing. U-M researchers are working to accelerate the efficiency of downstream genome and microbiome analysis. | Credit: Reetuparna Das
Seeding finds a set of candidate locations in the reference genome where a read can align. Possible matches are known as hits in the reference. In seed extension, for a read, the reference strings at the hit positions are matched at the read. With current technology, this takes hundreds of CPU hours for a whole genome.
For seeding, the researchers discovered a huge memory bandwidth bottleneck. They did hardware/software codesign and developed a new algorithm, data structure, and index that trades off memory capacity for memory bandwidth. They then built a custom accelerator that traverses the new index efficiently to find hits and seeds. The seeding algorithm has been released as open source software and is planned to be integrated with state of art alignment software from Broad Institute and Intel.
For seed extension, they built a systolic array that would in a few hundred cycles use approximate string matching to match read and reference data.
The researchers have developed a custom ASIC to eliminate the throughput bottleneck by using a pruning algorithm to optimize the alignment of DNA reads and candidate mutations and by reducing floating point computation by 43x when tested on real human data.
These enhancements and others have been mapped to custom hardware. This includes an accelerator for seed extension which achieves 2.46M reads/second, a ~1800x performance improvement, and a 27x smaller silicon footprint compared to a Xeon E5420 processor.
According to the researchers, when run on a high-end 56-core server in the Amazon cloud, their secondary analysis tools will take about six hours for whole genome sequencing. On an Amazon FPGA server, this reduces to about 20 minutes. When run on the researchers' custom hardware, processing time is about a minute.
The team has also developed techniques to optimize the read process for pathogen detection. One is to quickly analyze the beginning of a read to determine if it is host or pathogen material. If it is host, the remainder of the read can be skipped since it is only the pathogen material that is of interest. In addition, the researchers are often able to accomplish this host vs. pathogen differentiation using machine learning on squiggle data, without the need for resource-intensive basecalling.
Microbiome analysis to provide faster insights
When processing clinical samples, a fast data processing pipeline is key to the delivery of actionable insights.
"In clinical samples, much of the data—sometimes as much as 90%—can be host DNA, rather than microbial DNA," says Meera Krishnamoorthy, a Ph.D. student working with Wiens. "As a result, existing metagenomic classification tools store a lot of information about the host, and this can get computationally inefficient."
In collaboration with a team of researchers in Michigan Medicine and the School of Public Health, Wiens and Krishnamoorthy are working on in-silico machine learning approaches to host depletion, or the removal of host data reads, which will become a part of Das, Blaauw, and Narayanasamy's custom hardware. Their goal is to remove all of that host data before classification allowing downstream microbiome analyses to focus solely on microbial data. Existing host depletion methods are laboratory based and can be resource intensive to perform.
In contrast, Krishnamoorthy and Wiens' approach is computational and does not rely on large reference databases, but instead is based on a convolutional neural network. It takes as input read output by the basecaller and then after a series of convolutions and pooling steps outputs a prediction regarding whether or not the read pertains to the host. The proposed approach proposes to increase the efficiency of downstream analyses, enabling microbiome research that has the potential to transform future medical care.
Friday, January 08, 2021
IPhone12 will stop your implantable defibrillator
by John Hewitt , Medical Xpress
In a recent paper in the journal Heart Rhythm, doctors describe how they turned off the potentially life-saving cardiac defibrillator function of an implanted Medtronic device simply by holding an iPhone 12 near it. The authors had nothing personal against Medtronic, or for that matter, against the new iPhone. The main reason they singled the phone out here was because it is compatible with some of the most advanced new technologies available for various magnetic-based communications and charging.
08 jan 2021--Thistechnology, known as MagSafe, is basically harmless. It typically integrates charger, magnetometer and NFC reader into a compact package that depends on fairly decent alignment for efficient operation. The problem, at least for Medtronic, is the magnets that facilitate the positioning and docking. The iPhone 12, for example, has a ring of them around its central charging coil. In a nutshell,permanent magnetsare never going away, they are simply a perfect solution to many gadget problems. Applications including securing cochlear implant links, joining cables and fastening wristbands now make extensive of use of strong, miniature magnets.
Unless companies like Medtronic get on board and move to smarter device configuration options, they will continue to butt heads with consumer devices—and they will continue to lose. Smarter options don't have to be expensive; just look at your cheap IR TV remote or ultrasonic receiver-emitter pair. These devices simply work. They use an uncomplicated code to make sure there is no interference from all the other ambient sources that are invariably present. A couple of secure ultrasonic bits superimposed on your basic 40 khz carrier waves is all that is really needed. It is likely that companies like Medtronic are working on solutions like this; for example, a Medtronic programming head of some sort can be had on Ebay at the moment for a mere $34.99.
In the larger scheme of things, having a handy iPhone, iWatch, fitbit, or even JUUL vape pen in your pocket to turn off inappropriate pulses or change stimulation modes is not such a bad thing, considering the alternative. Note that all these devices have accidentally toggled pacemakers. For example, if you have say, a standard issue Medtronic c Implantable Cardioverter Pacemaker or Resynchronization Defibrillator, they don't give you a tiny pen. Instead, you lug around their giant 3" diameter,5/8" thick donut magnet that gives a field of 90 Gauss at 1.5."
Perhaps now is a good time to look a little closer into what different implantable pacemaker/defibrillators actually do, and why inappropriately triggering them—or not triggering them, as the case may be—is undesirable. Inappropriate triggering is nothing unusual; it is, in fact, the central preoccupation for these devices. In other words, choosing when to force a contraction, or rhythm, and when to let the heart try to take some responsibility. There are different ways to implant, record from, and stimulate an ailing heart. You can do it externally to the heart chambers, inside the atrium, the ventricle, or both depending on the condition or pathology.
For example, with permanent chronic atrial fibrillation you might get by with a single atrial lead, while with intermittent or paroxysmal fibrillation, you likely want dual atrial and ventricular leads. In pacemaker vernacular, common control modes have names like AOO (asynchronous atrial pacing), VOO (asynchronous ventricular pacing), or DOO (asynchronous A+V pacing). More advanced modes, like DDD mode, have additional logical if-then control, something like the following: "dual-chamber anti bradycardia pacing; if atria fails to fire, it is paced. If the ventricle fails to fire after an atrial event (sensed or paced) the ventricle will be paced."
For the case of the accidental activation by a smartwatch, researchers replicated the misbehavior using a Medtronic Visia AF MRI S DF-1 single chamber ICD defibrillator. In the case of the accidental activation by a JUUL case, a man with a prolonged H-V interval had a dual-chamber Medtronic Evera MRI XT DR DDMB1D1. The reporting authors noted that although in this case, he was fine after reverting to magnet mode and halting emergency stimulation, there is clear potential for unintentional temporary programming and arrhythmic complications with these devices as they stand now.
More information: Joshua C. Greenberg, et al. Life Saving Therapy Inhibition by Phones Containing Magnets, Heart Rhythm. DOI: doi.org/10.1016/j.hrthm.2020.12.032
Wednesday, January 06, 2021
Memorable music could reduce anxiety amongst elderly during COVID vaccinations, says researcher
Care providers should play music during the administration of coronavirus vaccinations to reduce feelings of anxiety in the elderly, researchers have said.
06 jan 2021--Research by Birmingham City University academic Mark Brill with Pendine Park Care Homes in Wales found that usingmusicat the point of care can reduce stress, particularly for those living with dementia.
"Our research with care homes has shown how powerful music is in supporting people living with dementia, making care tasks easier, so it feels like a natural extension to use it during vaccination," explained Mark Brill, a senior lecturer in digital innovation at Birmingham City University.
Brill worked alongside Manchester Metropolitan University's Dr. Stuart Cunningham and Dr. Harry Whalley from the University for the Creative Arts in the wellbeing study.
Through published research, the team have shown that playing appropriate music during care activities can have a significant impact in managing anxiety and agitation and make care easier to provide.
The peer reviewed study showed that memorable songs can cut through anxiety, open up communication and create a relaxed atmosphere where effective care can take place.
"Care homes are under increased pressures, yet something as simple as music can bring relief all-round," added Mark. "We have prepared guides and support materials which would help make it easy for care staff and clinicians to use the technology during the vaccination process."
More information: Stuart Cunningham et al. Assessing Wellbeing in People Living with Dementia Using Reminiscence Music with a Mobile App (Memory Tracks): A Mixed Methods Cohort Study, Journal of Healthcare Engineering (2019). DOI: 10.1155/2019/8924273
Provided by Birmingham City University
Saturday, January 02, 2021
Unique susceptibility to unique Sars-CoV-2 variants and vaccines
by John Hewitt , Medical Xpress
Credit: Wikipedia
Individuals with different genetic variants in their immune system components often have very different immune responses to Sars-CoV-2. They also will have different responses to vaccines. By the same token, newly emerged variants in Sars-Cov-2 can elicit different immune responses in identical immune systems. In the larger reality we are now dealing, potential variation in all the above must be simultaneously considered.
02 Jan 2021--We recently discussed several sources of newly uncovered variation inimmune genesthat control susceptibility to Sars. For example, modern humans with throwback versions of theneanderthalgene DPP4, or the spike protein cleaving protease TMPRSS2 appear to be at high risk for severe Covid. Other variants, like a highly-expressedTMEM1Bgene common in East Asians, or in genes of the heparin sulfate synthesis pathway, help explain the disproportionate severity of COVID-19 in some populations
Two papers, one recently published in Nature Immunology, and the other in Science, now extend the emerging gene list to include variations in the structure of the antibodies that are elicited by virus or vaccine. These variations include a particular kind of posttranslational modification of the anti-RBD (receptor binding domain) of the abundant IgG1 subclass known as afucosylation. What this essentially means is that for one reason or another, the afucosylated antibody is missing the addition of a fucose sugar molecule at a key structural location.
To better visualize the effect of this situation consider the above picture of the standard issue IgG antibody molecule. The variable portion, the arms of the Y shaped molecule, is known as the Fab region and it contains the epitopes that interact with the virus spike protein. The singular base region contains the constant Fc fragment, and incidentally, the glycosylated adornment hanging off of position N297 that potentially contains the fucose. In an almost fractal-like idiosyncrasy, this glycoform piece of kit also has a similar biantennary structure to the parent antibody, only on a much smaller scale, and with various sugars instead of amino acids. The fucose itself hangs off the stem portion of the aggregate glycoform, much as these glycans in turn hang on the antibody.
For anyone familiar with a related type of posttranslational modification known as ubiquitination, the N-glycan linkages form a kind of a code, much like the so-called ubiquitin code. Whereas the ubiquitin code consists of linear and branching subunits of variously phosphorylated or acetylated ubuitins, SUMOs, or NEDDs, the N-glycan code is composed of a heptasaccharide core which can be further extended with core fucose, terminal galactose (Gal), terminal sialic acid (Sia), and bisecting GlcNAc through selective enzymatic glycosylation reactions.
What the authors of these new papers found is that patients with severe forms of Sars-CoV-2 had increased likelihood of IgG1 antibodies with afucosylated Fc glycans, particularly in males. The net result of afucosylation proved to be enhanced interaction and binding with the immune activating Fcγ receptor, FcγRIIIA. This subsequently increases production of cytokines like interleukin-6 and TNF by monocytes. It should be noted that the canonical Fc receptors for human IgG include both activating (FcγRI, FcγRIIA, FcγRIIC, FcγRIIIA, and FcγRIIIB) and inhibitory (FcγRIIB) receptors. Most immune effector cells coexpress both activating and inhibiting FcγRs and therefore the net outcome of IgG interactions can often be predicted as the ratio of the binding affinities of a specific activating to inhibiting IgG receptors.
The way the authors figured this kind of stuff out was to first isolate the relevant IgG from a patient's serum using protein purification and tryptic digestion. Then nanoscale liquid chromatography coupled to tandem mass spectrometry is generally used to characterize the sites of potential glycosylation. But what the authors really wanted to get at was a more quantitative description of how much receptor binding is affected by afucosylation. To do this, various tried-and-true biophysical techniques including Surface Plasmon Resonance (SPR), Isothermal Titration Calorimetry (ITC), Microscale Thermophoresis (MST), and Biolayer Interferometry (BLI) are now available.
The authors of the Nature paper choose to use Biolayer Interferometry, which yielded graphs for binding (in nm units) as a function of time from which they could derive kinetic constants. BLI is an optical, label-free technique that analyzes the interference pattern of white light reflected from two surfaces. One is a layer of immobilized protein on the biosensor tip while the other is an internal reference. When a ligand immobilized on the biosensor tip surface binds to an analyte in solution there is a shift in the interference pattern that can be measured in real-time.
Afucosylated IgG was found to have a 20–40-fold increase in affinity to FcγRIIIa. This helps explain observed shifts in the front-line lung scavengers expressing FcγRIIIA, namely the alveolar macrophages, into an activated state of antibody-dependent cellular phagocytosis. While lowered Fc fucosylation is seen in the anti-Spike responses of the ARDS patients, other research has found that high levels of fucosylation are found in several kinds of cancer. In attempting to generate high-titer convalescent immunoglobulin treatments, it is likely important that plasma enriched in fucosylated anti-SARS-CoV-2 antibodies should be used. Although afucosylated IgG formed against viruses generally mediate stronger FcγRIIIa responses, they will often amplify cytokine storm and immune pathology.
While variants in the many genes that help build glycan chains, like for example the fucosyltransferase FUT2, might be expected to play a role in patient responses, perhaps an ever more pressing concern is differences in the antibody response to vaccines. In a brief spate of good news, the actual sequence of the new Pfizer mRNA vaccine was generously released unto the masses. The quickest to respond and attempt to decode this revelation was a guy named Bert Hubert, who quickly broke it down for us.
The main difference in the vaccine code is that uracil has been replaced by 1-methyl-3'-pseudouridylyl, which is labelled as Ψ. Although Ψ does not arouse the ire of our immune systems, it is still accepted as a normal uracil by the translation, transcription, and replication machinery of the cell. The other curious features are the substitutions of two prolines to stabilize the spike structure, and the deployment of special 5' and 3' untranslated regions before and after the main spike sequence. Bert has promised to release a second deep dive into the sequence in a few days, which is no doubt anxiously awaited by many.
More information: Saborni Chakraborty et al. Proinflammatory IgG Fc structures in patients with severe COVID-19, Nature Immunology (2020). DOI: 10.1038/s41590-020-00828-7
Mads Delbo Larsen et al. Afucosylated IgG characterizes enveloped viral responses and correlates with COVID-19 severity, Science (2020). DOI: 10.1126/science.abc8378
A year of blursdays: how coronavirus distorted our sense of time in 2020
Does it feel like 2020 went on forever? Did lockdown drag, and can you even remember how you spent your time when you weren't living under coronavirus restrictions? You are not alone. For many, 2020 has been the year in which the constancy of time was lost to the upheaval of coronavirus.
02 jan 2021--Objectively, time passes at a constant, linear rate. Subjectively, however, time waxes and wanes with ouractivities and emotions. Sometimes, it flies by, other times it drags so slowly that it almost stands still.
This is backed up by research I conducted in April, which explored how the early months of the coronavirus pandemic had affected people's experiences of the passage of time. Of particular interest was how quickly time felt like it was passing during lockdown in comparison to "normal" (that long-ago time before lockdown).
I surveyed 604 people about how quickly time felt it was passing that day and that week in comparison to before the lockdown. Participants also answered questions about their mood, family life and how busy they were to give context on the factors, which made time more likely to speed up or slow down for different people.
Tempus fugit?
My results showed that there was widespread distortion time during lockdown, with more than 80% of people reporting that time felt like it was passing differently. But lockdown did not distort time in the same way for everyone. Instead, time sped up during lockdown for 40% of people and slowed down for the remaining 40%.
Why was this? My analysis suggests that the perceived speed of time during the day was affected by a person's age, how satisfied they were with their level of social interaction, how stressed they were and how busy they were. In general, the days passed more quickly for younger people who were socially satisfied, busy and experiencing low levels of stress. Conversely, the day passed more slowly for older people, particularly those over the age of 60, who were socially dissatisfied, stressed and lacking tasks to occupy them.
Similar patterns were observed for the subjective speed of the week. A fast week was associated with being younger and more socially satisfied, whereas a slow week was associated with being older and less socially satisfied.
A second unpublished study I conducted during the November lockdown revealed that, of the 851 people surveyed, more than 75% experienced distortion to time and 55% reported that the start of the first lockdown felt longer than eight months ago. A slower second lockdown was associated with shielding, dissatisfaction with social interaction and greater depression and boredom.
The UK is not alone in its loss of time during lockdown. Studies conducted in France, Italy and Argentina also show widespread distortion to the passage of time during periods of strict COVID-19 restrictions.
Unlike in the UK, in France and Italy lockdown passed more slowly than normal for most people rather than being split 40/40 as in my April study. As in the UK, however, boredom was an important predictor of time slowing down in Italy and in France. In France, time also passed more slowly with increasing sadness.
Emotions and time
Why does being older, bored, stressed and socially dissatisfied make time pass more slowly? This question is difficult to answer.
Unlike other senses, we don't have an obvious organ for time. Instead, time is experienced as part of other sensory inputs, such as sight and hearing, and this has made it difficult to identify precisely how the brain processes it.
One possibility is that when we are bored and socially dissatisfied we have lots of spare cognitive capacity and that we then use some of that capacity to increase our monitoring of time. This increased monitoring then results in time passing more slowly than normal, simply because we are more aware of time than normal. Another possibility is that the emotional consequence of lockdown altered the way the brain processes time.
In particular, the negative emotions associated with isolation, boredom, sadness and stress may have contributed to a slowing of time. However, inconsistent effects of depression and anxiety across studies suggests that the effect of emotion on time is complex.
So what of 2021? Will time regain its regular rhythm? It is difficult to say. With the first vaccines currently being deployed, we maybe more hopeful than ever that normality is just around the corner. The reality may be that normality is many months away.
Regardless, while we can't change the actual time it takes for the vaccination programme to be completed, there are some things which we can do to speed up the wait. By keeping busy, minimising stress, engaging in as much face-to-face or online social interaction as we can and by reducing our stress levels, we can help the journey back to normality pass more quickly than normal.

")