Anxious about speaking in online classes and meetings? Here are 7 tips to make it easier

Many parents and students are engaged in a daily routine of speaking to people via a camera on a computer, tablet or phone during COVID-19 restrictions. This often means finding a quiet place in order to ask a question, provide an answer or share an opinion with a virtual audience.
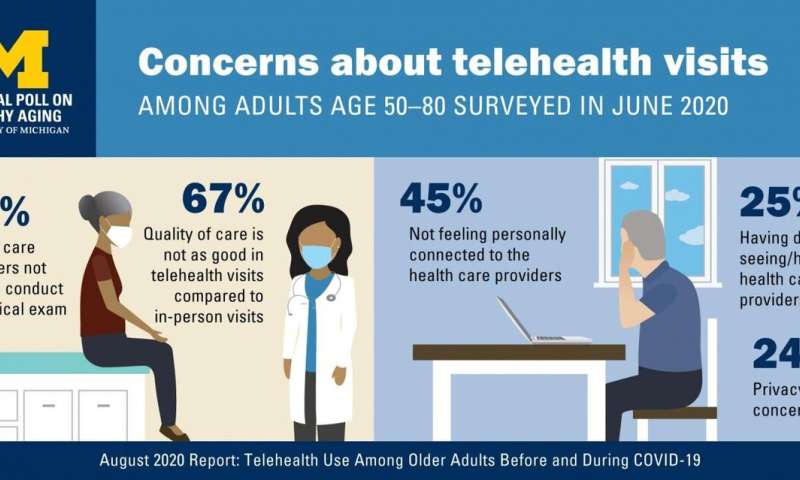
30 august 2020--Initial concerns about using video apps focused on privacy and equity issues.
Soon, new terms emerged such as Zoom fatigue. But an issue that has been less discussed is the role that nerves might play in these mediated sessions.
What is speaking anxiety?
For centuries, people have questioned their ability to speak in front of others. It's said the Roman orator Cicero (106-43BCE) turned pale and quaked before any speech he gave.
But it was in the 20th century that communication anxiety was studied in depth. It has been described by a number of different terms, including stage fright, unwillingness to communicate and communication apprehension.
Research suggests about one in five speakers experience high communication apprehension. This can make all speaking opportunities difficult.
Examples include speaking to a boss or teacher, contributing to a group discussion, or delivering a presentation. Public speaking anxiety is part of communication apprehension.
The prevalence of public speaking anxiety is well documented. It is complex (varying causes, indicators and treatment options), individual (affecting speakers differently) and unstable (changing levels of anxiety within and between presentations).
A focus on individual differences acknowledges that internal thoughts and feelings might not match external behavior. For example, a speaker who appears disengaged may actually feel a lack of control.
It is a tricky phenomenon. Some people can feel nervous the moment a speaking task is announced and, on the day of presentation, may rate themselves as more nervous than what an audience observes.
Nervous about the audience
It is the audience, and the potential for negative evaluation from that audience, that can make us feel anxious. And those listening can be physically or virtually present.
This brings us to the rather awkward situation of speaking to rows of little boxes on a screen in a video hook-up. Not only does this set-up limit broader non-verbal cues, but it also restricts general banter between participants.
On the plus side, this can make sessions more time-efficient, but it does tend to make conversations more stilted.
A perceived need to be visible is a contested area in online delivery. In educational settings, those who support "cameras on for everyone" suggest it helps to replicate usual classroom conditions, encourages discussion and ensures students are actually in attendance (not just logged on).
But it is important to consider the rationale behind making any feature mandatory. Participating via a video app is not the same as a live setting.
For a start, speakers rarely see themselves when talking to others. As a lecturer, seeing myself onscreen while speaking with a class can be distracting, especially when trying to look directly at the camera lens to maximize eye contact.
7 tips to make things easier
Whether running a business meeting or teaching a class, the following tips may help you to feel more comfortable speaking online:
- provide an agenda ahead of time, which could include sending out some prepared questions for discussion
- reduce uncertainty about participation by letting people know from the outset if there is any need or expectation to talk in a hook-up
- use linking statements and signposts to keep everyone on track as other cues and clues may be absent (walking across a room to a computer), so it's important to let all participants know what you are doing and why (for example: "I'm going to check the chat box at the end of this point so feel free to add any questions as I go along.")
- model good speaking practices, draw on simple structures to make your point and use language that is suitable for oral delivery
- rethink the value of calling on someone randomly to contribute to a discussion, because if people are worried they may be asked to respond without notice, they may be less likely to engage overall
- make decisions about the need for interaction (including break-out rooms) based on the type of session and number of participants, because needless interaction is not better than no interaction
- plan for each online event rather than stick to a set of general rules. For example, is it always necessary for speakers to see each other onscreen? As most educators will tell you, just because a student is physically present that doesn't mean they are actively engaged.
Online tutorials, workshops and meetings are here to stay for the moment. To create safe, supportive and productive sessions, we need to build competent and confident speaking practices.
Acknowledging that speaking anxiety is common, and affects people in live and virtual settings, is a good place to start.



")