Hospitalized patients with COVID-19 and abnormal sodium levels in the blood have an increased risk of experiencing respiratory failure or dying, according to a study published in the Endocrine Society's Journal of Clinical Endocrinology & Metabolism.
28 feb 2021--"This study shows for the first time that patients presenting at the hospital with COVID-19 and low sodium are twice as likely to need intubation or other means of advanced breathing support as those with normal sodium," said lead investigator Ploutarchos Tzoulis, M.D., Ph.D., M.Sc., Honorary Associate Professor in Endocrinology at University College London (UCL) Medical School in London, U.K.
Additionally, the researchers found that patients who develop high sodium levels during the hospital stay were three times more likely to die than those who have normal sodium levels throughout hospitalization.
"Sodium measurements can inform doctors about which COVID-19 patients are at high risk of deterioration and death," Tzoulis said. "Sodium levels can guide decision making about whether a COVID-19 patient needs hospital admission or monitoring in the intensive care unit."
Sodium is routinely measured as part of bloodwork done for all patients coming to the hospital, and its measurement is inexpensive, Tzoulis noted. Sodium is an essential mineral and helps regulate fluid volume in the body and blood pressure.
The study was conducted in 488 adults with COVID-19 admitted to two London hospitals, UCL Hospital and Whittington Hospital, over an eight-week period last year. The 277 men and 211 women had a median age of 68 years. They had a median hospital stay of eight days.
Nearly 32 percent of COVID-19 patients with low sodium levels at admission needed a breathing tube and ventilator or oxygen through a face mask compared with only 17.5 percent of patients whose sodium values were normal, the investigators reported. Unlike excess sodium in the blood, low sodium levels had no association with an increased risk of dying in the hospital, Tzoulis said.
Among patients with high sodium levels at any time during their hospital stay, nearly 56 percent died versus about 21 percent of patients whose sodium remained normal, the data showed.
Doctors usually treat high sodium levels with intravenous fluids, and low sodium may require intravenous fluids, fluid restriction or medications. However, both conditions are often underestimated and undertreated, Tzoulis said.
Fluid losses due to diarrhea, vomiting, sweating, and not drinking enough water can lead to high sodium levels. Therefore, Tzoulis stressed the importance of avoiding dehydration during a hospital admission for COVID-19.
More information: Ploutarchos Tzoulis et al. Dysnatremia is a predictor for morbidity and mortality in hospitalized patients with COVID-19, The Journal of Clinical Endocrinology & Metabolism (2021). DOI: 10.1210/clinem/dgab107
Journal information: Journal of Clinical Endocrinology & Metabolism
New machine learning tool facilitates analysis of health information, clinical forecasting
Clinical research requires that data be mined for insights. Machine learning, which develops algorithms to find patterns, has difficulty doing this with data related to health records because this type of information is neither static nor regularly collected. A new study developed a transparent and reproducible machine learning tool to facilitate analysis of health information. The tool can be used in clinical forecasting, which can predict trends as well as outcomes in individual patients.The study, by a researcher at Carnegie Mellon University (CMU), appears inProceedings of Machine Learning Research.
28 feb 2021--"Temporal Learning Lite, or TL-Lite, is a visualization and forecasting tool to bridge the gap between clinical visualization and machine learning analysis," explains Jeremy Weiss, assistant professor of health informatics at CMU's Heinz College, who authored the study. "While the individual elements of this tool are well known, their integration into an interactive clinical research tool is new and useful for health professionals. With familiarization, users can conduct preliminary analyses in minutes."
Time is a key part of clinical data that are collected in health care delivery. For example, during discussions of patients on rounds, in which doctors visit hospital patients to determine how they are doing, medical staff use visual aids that depict measurements of progression and recovery. Since electronic health records have been widely adopted, significant advances have been made in visualizing clinical data as well as in clinical forecasting. Yet a gap remains between the two.
TL-Lite begins with visualizations of information from databases and ends with visual risk assessments of a temporal model. Along the way, users can see the effects of their design choices through visual summaries at the levels of individuals as well as groups. This allows users to understand their data more completely and adjust machine learning settings for their analysis.
To show how the tool can be used, Weiss demonstrated the model with three electronic health records pertaining to three health matters: predicting severe thrombocytopenia (having abnormally low levels of platelets in the blood) during stays in the intensive care unit (ICU) among patients with sepsis, predicting survival of patients admitted to the ICU one day after admission, and predicting microvascular complications of type 2 diabetes among patients with the illness.
"The central goal of TL-Lite is to facilitate well-specified and well-crafted predictive forecasting, and this visualization tool is meant to ease the process," says Weiss. "At the same time, organizing the clinical data stream into meaningful visualizations can be aided by introducing machine learning elements. These approaches are complementary, so leveraging the benefits of one where another hits roadblocks results in a better overall solution."
Increasing glutathione levels lowers Alzheimer's pathology and improves cognitive decline
by CHeBA
Credit: Unsplash/CC0 Public Domain
Australian researchers have shown that a dietary supplement that increases the levels of a powerful antioxidant in the brain may represent a novel strategy for the treatment and/or prevention of cognitive impairment and debilitating neurodegenerative diseases such as Alzheimer's disease.
24 feb 2021--Findings of the study were recently published inNeurochemistry International.
A team of researchers from UNSW Sydney's Centre for Healthy Brain Ageing (CHeBA), and the School of Biotechnology and Biomolecular Sciences (BABS), has shown that dietary supplementation with glutathione precursor γ-glutamylcysteine (γ-GC), marketed as GlyteineTM, reduced oxidative stress, neuroinflammation and amyloid pathology in the brains of transgenic mice, a murine model to study Alzheimer's disease. The study also found significant cognitive improvements in the mice as determined using the Morris water maze, a test often used to test memory in mice.
The study identifies for the first time that γ-GC as a glutathione-elevating strategy in an Alzheimer's disease mouse model and is likely to have clinical relevance.
Lead author and Leader of CHeBA's Brain Ageing Research Laboratory, Dr. Nady Braidy, said: "Cellular depletion of glutathione has been linked to cognitive decline and the development of Alzheimer's pathology. Supplementation with γ-GC can transiently augment cellular glutathione levels by bypassing the regulation of glutathione homeostasis."
More information: Yue Liu et al. Supplementation with γ-glutamylcysteine (γ-GC) lessens oxidative stress, brain inflammation and amyloid pathology and improves spatial memory in a murine model of AD, Neurochemistry International (2020). DOI: 10.1016/j.neuint.2020.104931
Provided by CHeBA
Older people often incorrectly assume medicines don't have potential side effects
The findings suggest that physicians should spend more time explaining medication side effects to ensure their older patients are fully informed. Credit: University of California, Los Angeles
Older people correctly ascertained basic information such as dosage and duration of use for more than 70% of the medications they were prescribed, regardless of whether their physician explained it during an office visit. But when physicians failed to verbally provide information about potential side effects, people incorrectly assumed that about 55% of their prescribed medications had none. And even when physicians did discuss possible side effects, their patients incorrectly assumed there were no side effects for 22% of the medications.
24 feb 2021--There is a shortage of data about how well people understand basic information about the medications they are prescribed. This information is important for ensuring that people take their medications safely and properly and adhere to medication regimens.
The researchers examined data from 2009 and 2010 for 81 people age 50 and older who were subjects in a previous study aimed at improving how physicians communicate about newly prescribed medications.
The researchers note that more than half of the people in the study had high levels of health literacy and at least some college education. Also, people were allowed to refer to information that had been provided to them about the medications when they were responding to the survey. These factors may limit the applicability of the findings to the general population.
The findings suggest that although physicians might not need to spend much time conveying information on dosage, the number of pills in a prescription or how frequently medications must be taken, they should spend more time explaining side effects to ensure their older patients are fully informed.
Gaps in knowledge about side effects may put people, particularly older people, at risk for medication nonadherence. Patients may be less likely to take or continue taking medications if they discover the existence of potential adverse effects without having the opportunity to discuss those side effects with their physicians in a timely manner.
More information: Timothy Ho et al. Post-Visit Patient Understanding About Newly Prescribed Medications, Journal of General Internal Medicine (2021). DOI: 10.1007/s11606-020-06540-4
Provided by University of California, Los Angeles
Communal activities boost rehabilitation for older adults in long term care
Participants cleaning and watering. Credit: Tohoku University
A group of researchers has developed a new program showing participation and activity is critical for the rehabilitation of older adults in long-term care.
24 feb 2021--The results of their research were published in the journalPLOS ONEon February 12, 2021.
"Our study shows participatory programs that encourage elderly patients to be active need greater emphasis in elderly care centers," said Yoshihiko Baba, lead author of the study.
In 2015, the Ministry of Health, Labour and Welfare of Japan launched a comprehensive plan to care for the country's aging population. Crucial to this was rehabilitation centered on promoting activities that elderly patients could actively take part in.
Baba, a former graduate student at the Department of Internal Medicine and Rehabilitation Science at Tohoku University Graduate School of Medicine, and his supervisor, professor Masahiro Kohzuki, developed a program that fostered participation in activities such as park cleaning, gardening, and shopping. The program was implemented at 13 small-scale multifunctional at-home care (SMAC) facilities in Adachi Ward, Tokyo and was called the Adachi Rehabilitation Program (ARP).
A round of ARP comprises four weekly sessions. In the first session, participants take a bus to buy cleaning tools and seeds. In the following three sessions, they spend one-hour cleaning and maintaining flower beds in a nearby park. Participants are also encouraged to go to the park outside of the sessions.
Participants get off a bus to purchase cleaning tools and seeds. Credit: Tohoku University
The Japanese long-term care insurance system designates the amount of care needed according to seven levels: those at level one require a minimal care, while those at level seven require chronic care. ARP focused on those at the lower end of the spectrum.
Baba and his team conducted a controlled study for three courses (12 weeks) of ARP at the SMAC facilities.
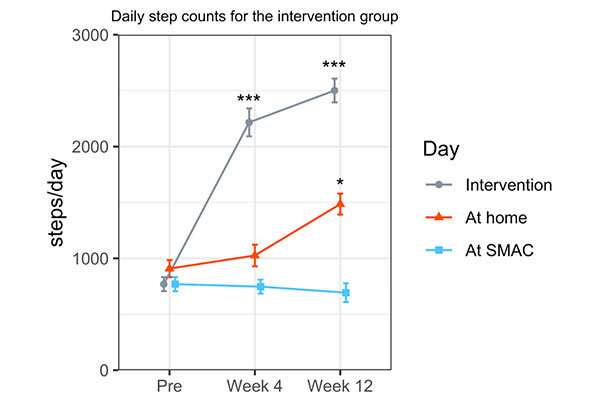
The daily step counts for participants. Credit: Tohoku University
As expected, step counts increased on days participants ventured out to parks and shopping centers. However, the research team also discovered that participation in ARP increased participants' step count even on days where there were no sessions.
ARP may have led to a behavioral change in which those under-long term care became more motivated to go out," added Baba. "Ultimately, community rehabilitation in long-term care insurance services can improve the physical activity of older adults."
More information: Yoshihiko Baba et al. Effects of Adachi Rehabilitation Programme on older adults under long-term care: A multi-centre controlled trial, PLOS ONE (2021). DOI: 10.1371/journal.pone.0245646
Provided by Tohoku University
Researcher offers lessons learned from a pre-pandemic study of telemedicine use
With the onset of the COVID-19 pandemic, telemedicine has become a new norm for many routine and non-emergency medical needs. But there are lessons to be learned from telemedicine's use—or lack thereof—prior to the pandemic, and a new study from a UConn School of Social Work researcher offers insight for policymakers, administrators, and public health officials when considering the implementation of new services.
24 feb 2021--A qualitative researcher, lead author and licensed clinical social worker Kelsi Carolan was brought into the study—which was conducted in 2017 and 2018 and was recently published in theJournal of Medical Internet Research—to examine the adoption of a telemedicine program in a California independent senior living community.
"Initially, the study was purely looking at stats, seeing what the effects of this intervention would be, if any, on the unnecessary use of emergency transport—residents being transferred to the emergency department," Carolan says. "What my co-authors were seeing in the numbers was that it wasn't having much of an effect. The intervention didn't seem to be working."
Despite the fact that the program was being offered at no cost to residents, and despite a push from the community's administration to utilize the program for cases that were not medically urgent, telemedicine wasn't actually reducing the number of emergency room visits amongst residents in the community. The intervention uptake was low, and the researchers wanted to better understand why.
Carolan and her co-authors conducted separate focus groups with frontline, emergency-trained staff members and with residents from the community. The residents included both individuals who had previously used the telemedicine option as well as those who had not. Overall, the residents expressed a desire to avoid emergency room visits as much as possible—they disliked the long wait times, financial costs, and potential health risks of visiting the emergency room.
Some residents said the telemedicine option had helped avoid an unnecessary trip, while another said that their telemedicine experience actually reinforced the need to go to the emergency room despite the resident's initial hesitancy—an unexpected benefit that helped diagnose a serious heart condition and ultimately led to important treatment.
The perceptions and experiences of the residents, however, were often in direct contradiction to the opinions of the community's frontline staff, who reported in their focus groups that residents were reluctant to use the telemedicine option and did not directly request it. The staff felt that telemedicine ultimately just delayed an otherwise inevitable trip to the emergency room, seeing it as an obstacle to providing care to the community's residents and not a valuable tool.
"Staff were saying it's not appropriate for emergency care, and most folks need to go to the emergency room," says Carolan, who has previously conducted qualitative research looking at a community paramedicine intervention. "It really made me think about my previous work and how much of a culture shift it is to ask emergency-trained responders, like EMTs and paramedics, to start to think about preventing emergency transport. Especially EMTs, because it's just not what they're trained to do. It's really asking a profession to change its whole culture and training."
The researchers ultimately concluded that a key barrier to the telemedicine program's successful implementation was this resistance from staff, though Carolan says the COVID-19 pandemic may well have helped to change those cultural perspectives within the profession.
"I have faith that people who go into emergency care careers, like EMTs—they really want to help people," she says. "There's room for change if there is increased recognition among these frontline providers that sending people to the emergency room unnecessarily is not actually helping them and may actually cause harm. There might be a broader and more mainstream understanding now of the risks, at least related to COVID, of going into the emergency room when it's not necessary."
Carolan says that, in addition to not measuring the potential impact of the pandemic on attitudes, the study's sample was limited to the voluntary participation of residents at only one independent senior living community, and that the community's residents were of higher socioeconomic status, which may have meant they had access to additional resources that rendered telemedicine less appealing.
But she says that, as a clinician, there's a lot for practitioners—and policymakers—to learn from the study.
"One of the things about the study that I find really interesting is that it really highlights how there can be such a discrepancy sometimes between the preferences of the people that we're serving as providers and what the providers, in this case the EMT staff, believe is best," she says. "In addition, we really have to think carefully when we're trying to introduce these kinds of interventions—which is not even really specific to telemedicine -about the people who are on the ground actually trying to provide them. It's one thing for me to come in, as a researcher, or for these big intervention or demonstration projects to be put in place, but if the people on the ground who are actually in charge of delivering the intervention don't feel it is valuable or a good use of their time, then the whole thing may be destined to fail. For me, that encourages caution."
She says the study also highlights the importance of qualitative research in providing a more complete look at the effectiveness of policies and interventions.
"If we just looked at the quantitative data, the stats of the study, we would not really understand the full picture; we would just know that the telemedicine intervention wasn't really successful," Carolan says. "That's what it looks like with just the numbers. And I think what the study actually highlights is that it wasn't the full picture—the lack of uptake was related to the lack of provider buy-in."
She continues, "Often when people think about qualitative research, the thought is that it's not necessarily as relevant to policymaking as quantitative data because they think, 'Well, it's not representative. We can't extrapolate about the whole population from it.' But sometimes you're really losing an important part of the story when you aren't actually talking directly to people about what's going on."
More information: Kelsi Carolan et al, Use of Telemedicine for Emergency Triage in an Independent Senior Living Community: Mixed Methods Study, Journal of Medical Internet Research (2020). DOI: 10.2196/23014
Journal information: Journal of Medical Internet Research
Study demonstrates the effectiveness of raloxifene in treating inflammatory processes associated with COVID-19
by Universitat Politècnica de Catalunya · BarcelonaTech (UPC)
Colorized scanning electron micrograph of an apoptotic cell (green) heavily infected with SARS-COV-2 virus particles (yellow), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. Credit: NIH/NIAID
Researchers from the UPC's Molecular Biotechnology Centre show that a drug for osteoporosis called raloxifene may inhibit molecules involved in the inflammatory processes associated with COVID-19.
24 feb 2021--About 20% of COVID-19 patients have a severe clinical picture and require intensive care. These patients develop varying degrees of pneumonia that may evolve to more severe stages and cause organ dysfunction. Patients with severe symptoms exhibit elevated levels of proinflammatory molecules, a reaction known as cytokine storm. Recently, scientists have found that an inflammatory mediator known asbradykininmay trigger this inflammatory process that is observed in patients with severe COVID-19and that can be deadly.
In the fight against the disease, researchers are turning to drug repurposing to quickly provide a therapy by using already existing drugs. In this context, the researchers Juan Jesús Pérez and Patricia Gómez-Gutiérrez, from the Molecular Biotechnology Centre and linked to the Department of Chemical Engineering of the Universitat Politècnica de Catalunya · BarcelonaTech (UPC), have been looking for drugs to prevent bradykinin signaling. Using virtual drug screening, they have discovered that raloxifene, a drug used for osteoporosis and certain types of breast cancer, can act as a bradykinin inhibitor.
The study was conducted using computer-aided molecular design. The principal investigator, Juan Jesús Pérez, a professor at the Barcelona School of Industrial Engineering (ETSEIB), says, "We have performed drug screening using computer-aided drug design methods. After identifying the compound in silico, we sent a sample to an external laboratory for its in vitro characterisation, which corroborated its new pharmacological profile, and raloxifene has been shown to act as a partial agonist of bradykinin."
The conclusions of this research are set out in the article Discovery of a bradykinin B2 partial agonist profile of raloxifene in a drug repurposing campaign, which was published in the scientific journal International Journal of Molecular Sciences.
The increased availability of bradykinin in severe COVID-19 patients could be the trigger for cytokine storm. This hypothesis relies on the downregulation of angiotensin converting enzyme 2 (ACE2), the gateway for SARS-Cov-2 into cells, in such patients. This new perspective suggests that inhibition of bradykinin signaling may be a suitable therapy to prevent cytokine storm and its consequences.
Currently, icatibant is the only bradykinin antagonist approved as a therapeutic agent for the treatment of hereditary angioedema and it is now undergoing a clinical trial to assess its benefits for the treatment of COVID-19 patients. In fact, preliminary results from a limited study suggest that inhibition of bradykinin signaling is associated with decreased oxygen requirements in COVID-19 patients.
Raloxifene undergoing clinical trial as an antiviral agent
The result of the study by UPC researchers supports other studies suggesting the suitability of raloxifene in COVID-19 patients, based on its capacity to inhibit another inflammation signaling pathway, and also for being a prospective antiviral agent against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
In the framework of a European project, the Exscalate4CoV consortium of supercomputing centers, including the Barcelona Supercomputing Center–Centro Nacional de Supercomputación (BSC-CNS), identified raloxifene, aimed at another therapeutic target, as an antiviral agent against SARS-CoV-2 in June 2020, also by using virtual screening techniques. Clinical trials are now underway in Italy to test its effectiveness in patients with mild symptoms.
Juan Jesús Pérez says, "The good results of the lines of research on raloxifene suggest that it is a good candidate drug against COVID-19."The researcher explains that "drug repurposing has long been used to discover new therapeutic uses for existing drugs, because it increases the chances that the compound can be used. In addition, clinical trials will not take as long as for a new drug, because its toxicity has already been tested."
More information: Patricia Gomez-Gutierrez et al. Discovery of a Bradykinin B2 Partial Agonist Profile of Raloxifene in a Drug Repurposing Campaign, International Journal of Molecular Sciences (2020). DOI: 10.3390/ijms22010257
Provided by Universitat Politècnica de Catalunya · BarcelonaTech (UPC)
Sunday, February 21, 2021
Machine learning can help doctors diagnose Parkinson's disease by looking at patients' movements
Immunohistochemistry for alpha-synuclein showing positive staining (brown) of an intraneural Lewy-body in the Substantia nigra in Parkinson's disease. Credit: Wikipedia
Scientists from Skoltech and A.I. Burnazyan Federal Medical and Biophysical Center have designed and developed a second opinion system based on AI-assisted video analysis that can help medical professionals to objectively assess patients with Parkinson's disease (PD), even at an early stage. This approach can help avoid misdiagnosing this disease, distinguishing between its stages, adjusting therapy and recommending diagnosed patients for deep brain stimulation surgery. The paper was published in IEEE Sensors Journal.
21 feb 2021--A growing number of people withneurodegenerative diseases, due to population aging, will mean that in the coming decades, humanity might face a bona fideParkinson's disease pandemic. PD, currently the fastest growing neurodegenerative disease, affects the patients' quality of life quite severely and needs to be diagnosed as accurately and as early as possible. The challenge there is to distinguish between Parkinson's and other diseases with similar motor symptoms, for instance, essential tremor. So far, PD has no single biomarker that could be used to diagnose it consistently, and doctors have to rely on their observations, which often lead to wrong diagnoses revealed in pathological examinations.
Assistant Professor Andrey Somov and his colleagues built a so-called second opinion system that uses machine-learning algorithms to analyze video recordings of patients performing specific motor tasks. In a small pilot study, this system showed a very high level of performance in detecting potential cases of PD and distinguishing it from essential tremor.
The system uses video recordings, making the diagnostic process fast, unobtrusive and comfortable for the patients. The team designed a set of 15 common exercises such as walking, sitting down on chair, standing up, folding a towel, filling a glass with water, and touching one's nose with one's index finger. These were general and finer movements, no movement at all (to assess tremor at rest) and some activities that clinicians use to evaluate the tremor.
"The exercises were designed under the supervision of neurologists and came from several different sources, including scales that are used for monitoring Parkinson's disease and previous research done in this area. Each exercise had a target symptom that it could reveal," Ekaterina Kovalenko, Skoltech Ph.D. student and a coauthor of the paper, explained.
In the pilot study, 83 patients with or without neurodegenerative diseases were recorded performing these tasks. The videos were then processed using a piece of software that places keypoints onto the human body corresponding to joints and other parts of the body, creating simplified models of moving subjects. Those were analyzed using machine learning techniques.
The team says that the use of video and machine learning introduces a certain degree of objectiveness into the diagnostic process, allowing researchers and doctors to detect very specific features of the disease and its stages which are not visible to the naked eye.
"Our preliminary results show potential in improving diagnosis with the help of video analysis. Our goal is to provide a second opinion for doctors and clinicians, not to replace them. A video-based method perhaps is the most convenient for patients, as it is the most versatile and noninvasive when compared to various sensors and testing," the authors write in their paper.
"Machine learning and computer vision methods we used in this research are already well established in a number of medical applications; they can be trusted, and the diagnostic exercises for Parkinson's disease have been in development by neurologists for some time. What is truly new about this study is our quantitative ranking of these exercises according to their contribution to a precise and specific final diagnosis. This could only be achieved in collaboration between doctors, mathematicians and engineers," Dmitry Dylov, Skoltech Associate Professor and coauthor of the study, said.
Inearlier studies, Somov's team also used wearable sensors in a similar feasibility study that helped them detect the most informative exercises for machine learning-assisted diagnosis of Parkinson's.
"As part of the research process, we had the opportunity to closely interact with doctors and medical personnel, who shared their ideas and experience. It was fascinating observing how two seemingly different disciplines came together to help people. We also had the opportunity to monitor all parts of the research, from designing the methodology to data analysis and machine learning," Kovalenko said.
"This collaboration between doctors and scientists in data analysis allows for many important clinical nuances and details that help achieve the best results. We as doctors see great potential in this; apart from differential diagnosis, we need objective tools to assess motor fluctuation in patients with PD. These tools can provide a more personalized approach to therapy and help make decisions on neurosurgical interventions as well as assess the outcomes of surgery later," neurologist Ekaterina Bril, a coauthor of the paper, noted.
Andrey Somov said the team's next goal is to combine video analysis and sensor data in the task of detecting PD and diagnosing its stages—they expect that this will improve accuracy. "We also keep in mind the innovation aspects of our work—our team agrees that it does make sense to consider converting our research results into an intuitive software product. We believe our joint research efforts will have a positive effect for the patients with PD," he added.
More information: Ekaterina Kovalenko et al. Distinguishing Between Parkinson's Disease and Essential Tremor Through Video Analytics Using Machine Learning: a Pilot Study, IEEE Sensors Journal (2020). DOI: 10.1109/JSEN.2020.3035240
Provided by Skolkovo Institute of Science and Technology
COVID-19 telemonitoring program helps reduce hospital admissions and ER visits
The rapid upscaling of a telemonitoring program in which health care providers performed daily telemedicine check-ins on COVID-19 patients faced a unique set of challenges. How these were resolved, and early outcomes, are reported in the peer-reviewed journal Telemedicine and e-Health.
21 feb 2021--"Kaiser Permanente's Virtual Home Care Program (VHCP) was able to rapidly establish a telemedicine-based program for the management of COVID-19 positive patients in the DC and Baltimore Metro regions. Preliminary data suggest that such a program may be effective in keeping patients out of the hospital and/or emergency room," stated James Shaw, MD, Med-Atlantic Permanente Medical Group, and coauthors.
The researchers described three main challenges. The constant flow of providers into and out of the program. Challenges in the management of Spanish-speaking patients and the need for translators. The initial lack of an alert system in the pulse oximetry program to alert patients and providers when a patient registered a low oxygen reading.
"The COVID-19 pandemic has provided an opportunity for telemedicine and telehealth to grow exponentially. Kaiser's work in the DC Metro area is a testament to providers developing and implementing new ways in rapid fashion in order to maximize health care delivery," says Charles R. Doarn, MBA, Editor-in-Chief of the Journal and Research Professor and Director of the Master of Public Health Program, Department of Environmental and Public Health Sciences, University of Cincinnati, Ohio.
More information: James G. Shaw et al, A Novel Large Scale Integrated Telemonitoring Program for COVID-19, Telemedicine and e-Health (2021). DOI: 10.1089/tmj.2020.0384
Provided by Mary Ann Liebert, Inc
Wednesday, February 17, 2021
5 things you need to know about the AstraZeneca vaccine
by Kirsty Wilson, Jennifer Boer and Magdalena Plebanski, The Conversation
Credit: Pixabay/CC0 Public Domain
The Therapeutic Goods Administration (TGA) yesterday announced it has provisionally approved AstraZeneca's COVID vaccine for use in Australia.
17 feb 2021--The approval applies to people over 18, including adults older than 65. The recommended interval between the two doses is 12 weeks, but the second dose can be administered a minimum of four weeks after the first.
We now have two vaccines provisionally approved, which is welcome news for Australia's vaccine rollout. Vaccinations with the Pfizer shot are set to begin next week, and we should see inoculation with the AstraZeneca vaccine start some time in March.
Here are five things to know about the AstraZeneca vaccine.
1. Storage and distribution
The Oxford/AstraZeneca vaccine, also known as ChAdOx1 nCoV-19, or AZD1222, is a viral vector vaccine. Scientists used an adenovirus, originally derived from chimpanzees, and modified it with the aim of training the immune system to mount a strong response against SARS-CoV-2 (the virus that causes COVID-19).
One key characteristic of this vaccine is that it can be stored at 2-8℃ (so, in a normal fridge). This is distinct from some of the other COVID-19 vaccines—such as Pfizer's mRNA vaccine—which must be stored at ultra-cold temperatures. So the AstraZeneca vaccine can be widely distributed with relative ease.
Additionally, AstraZeneca has multiple supply chains. Around the world they have multiple manufacturing sites, partners from whom to source ingredients, and distributors who can deploy the vaccine. These partnerships will accelerate production and distribution.
At this stage, the AstraZeneca vaccine will be the only locally available vaccine manufactured in Australia. Biotechnology company CSL has been working to upgrade its facilities so it can produce the vaccine locally at scale. It expects up to two million doses will be available by the end of March.
2. Safety and efficacy in people over 65
Phase 2 human trials tested safety and immune responses of the AstraZeneca vaccine, including in people over 65. The vaccine was found to be safe, showing just some mild and moderate reactions, and it induced similar immune responses across age groups.
Although the subsequent phase 3 trials included much larger numbers of people, they didn't include as many older people as trials for some of the other vaccines. So researchers couldn't confidently assess efficacy in this group at the time. Studies are ongoing, and there's still some uncertainty about the vaccine's efficacy in older people.
There are no specific safety concerns (especially based on overseas data) and the vaccine induces good immune responses, which is a positive indicator it could be effective in the elderly population. Therefore, the TGA has ruled the vaccine should be administered to elderly people "on a case-by-case basis" where the benefits outweigh the possible risks.
The person, their family and medical professionals might make the decision not to vaccinate if, say, the person is very elderly and frail, or has multiple medical conditions.
3. Timing of doses
In initial studies, the vaccine's efficacy was 62% with two standard doses. However, there was some variability depending on the dosage and timing.
Since then, scientists have asked questions about the optimal dose and interval. A preprint manuscript in The Lancet shows the vaccine demonstrated 82.4% efficacy after two standard doses three months apart. The efficacy was lower if the doses were closer together: 54.9% if the interval was less than six weeks.
Although this data is yet to be peer-reviewed, it suggests the timing between doses is a key factor in this vaccine's efficacy. The TGA has reflected this in its advice.
But will a person be protected already after one immunization, while waiting for the second boosting jab? The preprint study shows the vaccine has 76% efficacy after a single dose, when assessed over the first 90 days after vaccination.
4. Protection against different strains
As viruses mutate and give rise to new variants, this can affect how well certain vaccines work against them.
We've seen this with the B.1.351 variant of SARS-CoV-2, originally identified in South Africa. Following a multi-center clinical trial in South Africa, researchers concluded two doses of the AstraZeneca vaccine had minimal efficacy in mild to moderate COVID-19 cases, specifically due to the B.1.351 variant.
There's still hope the vaccine will be effective against more severe cases of COVID-19. But South Africa has halted the rollout of the AstraZeneca vaccine for now.
The news is looking better for the UK strain, B.1.1.7. In a phase 2/3 clinical trial in the UK, researchers concluded the AstraZeneca vaccine had an efficacy against the B.1.1.7 variant similar to that of other variants—74.6% compared with 84%. It's important to note this study is also a preprint, so it hasn't yet received the same scrutiny as other published research.
Interestingly, both the UK and South African variants have the same mutation—the N501Y mutation—but the south African variant has an additional mutation, E484K. Research shows this mutation contributes to the virus evading antibodies from COVID-19 patients against SARS-CoV-2.
5. Can it reduce transmission as well as disease?
This question has been asked of all COVID-19 vaccines, and emerging data for the AstraZeneca vaccine is encouraging. The Lancet preprint we mentioned earlier has shown this vaccine may block transmission after a single dose.
The researchers derived this data by taking weekly nose swabs from both symptomatic and asymptomatic cases and testing for the presence of the virus. (If a person has virus in their nose and are breathing it out, they're more likely to infect someone else.) They observed a 67% fall in swabs positive for the virus after one immunization.
In a separate preprint, people who received the AstraZeneca vaccine (as opposed to the placebo) and were swab positive showed reduced periods of viral shedding, which could also have a positive impact on transmission of disease.
This data suggests the AstraZeneca vaccine also has potential to substantially affect virus transmission, by reducing the number of highly infectious people in a population.
Provided by The Conversation
Tuesday, February 16, 2021
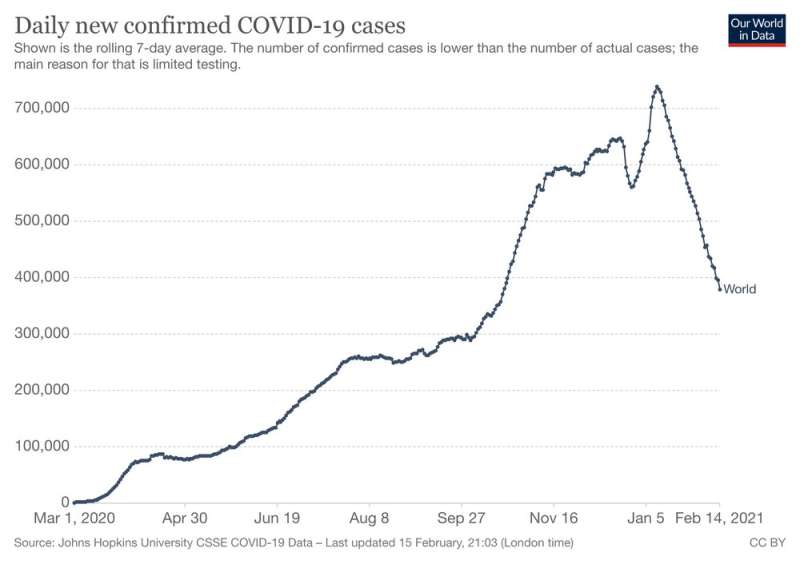
Global weekly COVID cases are falling, WHO says—but 'if we stop fighting it on any front, it will come roaring back'
The number of reported global weekly COVID cases is falling and has dropped nearly 50% this year, the World Health Organization (WHO) said overnight. This incredibly encouraging news shows the power of public health measures—but we must remain vigilant. Letting our guard down now, when new variants are emerging, could easily reverse the trend.
16 feb 2021--According to a WHOpress release: "Last week saw the lowest number of reported weekly cases since October", Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization (WHO) told journalists at a regular press briefing in Geneva.
Noting a nearly 50% drop this year, he stressed that "how we respond to this trend" is what matters now.
While acknowledging that there is more reason for hope of bringing the pandemic under control, the WHO chief warned, "the fire is not out, but we have reduced its size".
"If we stop fighting it on any front, it will come roaring back".
This welcome news shows that when governments respond rapidly by putting in place public health measures, we reap the benefits even before widespread vaccine rollouts. That's a really important message now, and for when the next pandemic hits (and another one eventually will).
As good as this news is, though, we are still seeing infections in fairly large numbers worldwide. And, as we have regrettably seen in the past, subsequent waves of infection can easily emerge.
We also now have a series of variants to contend with. Even as begin to understand how the variants now circulating will affect the effectiveness of current vaccines, it's possible we could see yet another new variant emerge that would reverse the downward trend. This remains a real risk when there are still so many new infections worldwide and when so few countries have been able to start vaccinating.
It's too early to see vaccine effect
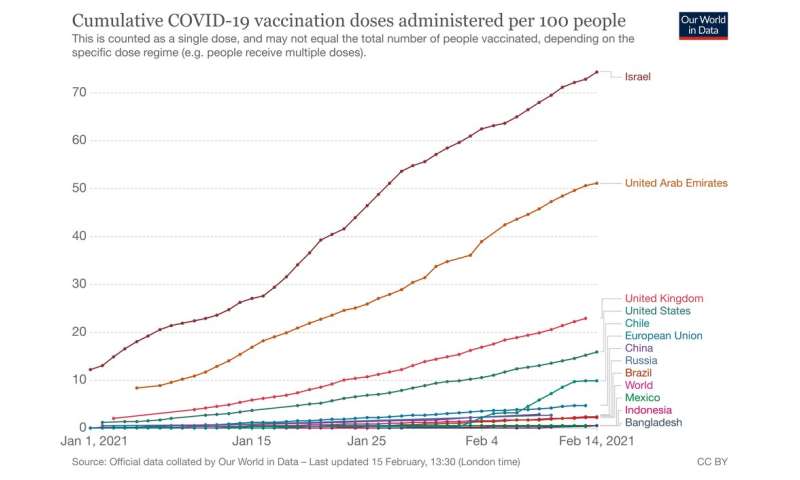
Some countries, such as Israel and the United Kingdom, have already vaccinated huge swathes of their population. That's a tremendous achievement and we will start to see the benefits in the coming months. But fundamentally, it's too early to see the effect of the vaccine rollout in widespread reduction of infection.
On the other hand, we have recently seen a much greater focus on public health measures in places such as Europe, the Middle East and the United States. These places have been significantly affected by COVID outbreaks and are dealing with third waves, as some are preparing for their fourth.
It's likely these public health measures—such as lockdowns, physical distancing, mask-wearing and increased hygiene measures—are what's driving the global downward trend. That shows the benefit when leaders do engage and bring their populations with them.
To keep that trend going in the right direction, we need high levels of public compliance with those public health measures and more equitable access to vaccines globally.
Unequal global access to vaccines is a major risk
Very few low-income countries have started a widespread vaccine rollout, and many are struggling to secure doses. Having unequal access globally to vaccines is obviously morally wrong and dangerous—but it also represents a great economic risk to high income countries like Australia.
Having high-income countries buying up all the stock of vaccines and leaving poorer nations with little recourse will prolong the pandemic. And that's bad news for the global economy, with estimates suggesting the pandemic will cost US$16 trillion dollars.
Even if Australia were able to maintain its success so far, having the pandemic run out of control in other countries means no travel, will continue to make it hard for Australians to return home, and could lead to shortages of products and materials from other countries. As the global financial crisis showed, economic strife in other parts of the world can have profound impact locally, even when Australia is doing relatively OK.
The risk this poses to lives and to the global economy is one reason the WHO has called for vaccine rollouts to begin in all countries in the first 100 days of 2021, and for health-care workers in lower- and middle-income countries to be protected first.
The WHO has issued a vaccine equity declaration calling for, among other things, world leaders to increase contributions to the UN-led vaccine equity initiative, COVAX, and to share doses with COVAX even as they roll out their own national campaigns.
As the WHO's Director-General said overnight, the fire is not out and "if we stop fighting it on any front, it will come roaring back".
That's why sticking to the fundamentals of infection control is so important. That means keeping up with the hand-washing and physical distancing. It means wearing a mask if you can't physically distance and complying with lockdowns and other public health orders. Yes, it's hard to maintain a high level of commitment, but the alternative is far worse.
When people start to hear that global case numbers are improving, there's a tendency to relax—and that's risky. Now is the time we need to work together to see this contained, and ideally suppressed.
We may never completely eradicate this virus. But if we stick with the public health measures, and vaccinate as many people as possible worldwide, we can keep the trend going in the right direction.






 heavily infected with SARS-COV-2 virus particles (yellow), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. Credit: NIH/NIAID")
 of an intraneural Lewy-body in the Substantia nigra in Parkinson's disease. Credit: Wikipedia")